Pediatric Tracheostomy
Pediatric Tracheostomy. M. Lauren Lalakea MD Chief, Otolaryngology/HNS, Valley Medical Center, San Jose, CA Clinical Associate Professor, Stanford. Tracheotomy--Introduction. Initially procedure of last resort to relieve airway obstruction, eg diphtheria, epiglottitis

Pediatric Tracheostomy
E N D
Presentation Transcript
Pediatric Tracheostomy M. Lauren Lalakea MD Chief, Otolaryngology/HNS, Valley Medical Center, San Jose, CA Clinical Associate Professor, Stanford
Tracheotomy--Introduction • Initially procedure of last resort to relieve airway obstruction, eg diphtheria, epiglottitis • High expectation for short duration, w decannulation • Indications expanded to include access for pulmonary toilet and assisted ventilation (polio) nathanclarkecommunication.wikispaces.com Uofmchildrenshospital.org
Tracheostomy--Introduction • Current trends: • ↓trachs for acute airway obstruction • ↑trachs for prolonged ventilation (>50%) • ↓decannulation rate: 28—51% • ↑trach duration: 2 yrs for those decannulated • Avg. age: 2—3 yr, >50% younger than 1 yr • Indications • Airway obstruction • Assisted ventilation • Pulmonary toilet
Indications • Airway obstruction • Congenital: • Craniofacial anomalies • Bilateral vocal cord paralysis • Tracheomalacia • Laryngeal anomaly • Neoplasm
Craniofacial Anomaly: Pierre Robinmicrognathia, glossoptosis, cleft palate php.med.unsw.edu.au
Bilateral Vocal Cord ParalysisHigh-pitched stridor, CNS etiology www.drninashapiro.com
TracheomalaciaInspiratory and expiratory stridor 2011.prepsa.courses.aap.org
Laryngeal Anomaly: Glottic Web wiki.uiowa.edu
Neoplasm: Lymphangioma openi.nlm.nih.gov
Indications • Airway Obstruction • Acquired: • Subglottic stenosis • Cricoid is a complete ring • ETT -->mucosal ischemia, necrosis • Perichondritis, cartilage injury • Progressive stridor, failed extubation • Trach if med and surgical management fail • Recurrent respiratory papillomatosis • Trauma emedicine.medscape.com
Indications • Assisted ventilation • Congenital central hypoventilation • Chronic lung dz, eg BPD • Neuromuscular disease • Pulmonary toilet • Neurologically impaired children • Recurrent respiratory infections, aspiration
Timing of Tracheotomy Controversial in pedi pts • Prolonged intubation → risk of airway injury • Incidence of subglottic stenosis low in neonates despite lengthy intubation • Meticulous NICU care • Pliable larynx and trachea • Older children and adults: • Consider trach after 2-3 wks of intubation • Consider likelihood that underlying process will reverse/improve
Pre-Trach Evaluation • Airway obstruction • Flexible laryngoscopy—dynamic evaluation • Rigid laryngoscopy and bronchoscopy with spontaneous ventilation • Any treatable conditions?
Pre-Trach Evaluation • Dynamic evaluation--laryngomalacia primehealthchannel.com
Pre-Trach Evaluation • Assisted Vent + Neurologic Dz • Discussion with 1° team, Pulmonary, family • Goals of care • All • Wt> 1500 gm, FiO2 <60% • Hct, coags • Informed Consent
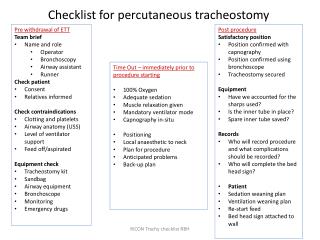
Tracheotomy Technique • General Anesthesia, with ETT • Vs. LMA or bronchoscope • Positioning with neck extended • Palpation of landmarks, incision marked • Pedi larynx is high, cricoid easiest to palpate • Horizontal or vertical incision below cricoid
Tracheotomy Technique • Midline dissected, thyroid isthmus divided • Stay sutures placed thru rings • Trachea opened vertically
Tracheotomy Technique • ETT is withdrawn slightly • Appropriate trach tube placed • Position and adequate ventilation confirmed • Tube size adjusted prn • Excessive leak • Excessive length
Tracheotomy Technique • Tube secured with sutures • Stay sutures labeled • Facilitate tube replacement in case of accidental decannulation • Twill tape used around neck to secure trach • Snugly tied to prevent dislodgement
Tracheostomy Variations • Vertical skin incision • Stoma ‘matured’ by suturing skin in 4 quadrants to edges of tracheal incision • Allows easier tube replacement if dislodged
Post-Operative Care • Transport directly to ICU • CXR to confirm tube position, r/o PTX • Sedation to minimize risk of accidental decannulation while stoma immature • Routine suctioning, humidified air • “Do not change trach ties” • Obturator, extra trach tubes at bedside • Same size, and one size smaller
Post-Operative Care • First trach change • At 5-7 days post-op • 2 ENT MDs • Neck extended, fresh tube placed • Stay sutures removed, ties changed • Confirms that stoma is sufficiently mature to allow future changes by non-surgical personnel • Sedation weaned, transfer out of ICU as appropriate
Post-Operative Care • ‘Hands-on’ caregiver training begins • Infants and young children vulnerable to trach catastrophe • Pedi trach tubes are single canula--require meticulous care • General trach care, suctioning technique • Trach tube changes—q 1-2 wk • CPR training • Discharge planning
Complications • Complication rates vary, up to 40—50% • Early: • Accidental decannulation • False passage, loss of airway • Potential for significant morbidity/mortality • ↓Risk with: • Adequate sedation/ immobilization • Appropriately sized and secured tube • Close monitoring and nursing care • Stay sutures +/- ‘mature’ stoma to facilitate tube replacement sciencedirect.com
Complications: Early • Tube obstruction/ mucus plugging • Potential for significant morbidity/ mortality in kids • Small diameter single canula, vulnerable age group • ↓Risk with: • Humidified air • Frequent suctioning • Appropriate monitoring • Pneumothorax/ pneumomediastinum 0.6 – 6% • Hemorrhage • Local infection, skin breakdown
Complications--Late • Tracheal granuloma—39% • Stomal, suprastomal, distal • ↓Risk with meticulous trach care, proper suctioning technique • Surveillance bronchoscopy, excision to maintain patency tracheostomy.com Utmb.edu
Complications: Late • Tube obstruction/ mucus plugging – 13% • Accidental decannulation—12% • Caregiver training is critical • Adequate monitoring and home support • Local infection – 9%
Complications: Late • Speech delay • Smaller trach size allows for better airflow and voicing • Passey-Muir valve appropriate for some • Early Start and Speech Tx
Complications: Late • Suprastomal collapse/ malacia – 8% • Tracheal or subglottic stenosis • Arterial erosion/ tracheal-innominate fistula • “Sentinel Bleed” • TE fistula--acquired readcube.com
Complications • Tracheocutaneous fistula: 11-42% • Persistent fistula after successful decannulation • ↑Risk if trach duration > 1 yr • 90% of ‘Starplasty’ trachs have TC fistula • May require surgical repair • Death • Trach-related = 0 – 3% • Accidental decannulation / mucus plugging most common • Overall = 8.5 – 19%
Trach Tubes: Which are Best? • Cuffed vs. uncuffed • Neonatal vs. pediatric • Bivona vs. Shiley • Single cannula vs. with inner cannula • Metal vs. plastic • Appropriate length and diameter? • Fenestrated Jackson Trach tube Cuffed Shiley Trach with Inner Cannula
Trach Tubes: Which are Best? • Fenestrated tube • Allows passage of air up thru vocal cords to facilitate speech • May ↑ aspiration risk • More prone to granulation tissue formation tracheostomy.com
Trach Tubes: Which are Best? • Ideal trach tube: • Soft enough to conform w/o pressure, injury, discomfort • Rigid enough to avoid collapse • Material causes minimal tissue reaction • Has inner cannula that can be removed and cleaned • Not available for plastic pediatric trachs • Has stylet or obturator to facilitate insertion • Bivona and Shiley meet most criteria
Trach Tube Size Guidelines Length • Neonatal vs. Pedi • Neonatal equivalent diameter vs. Pedi, but 5-8 mm shorter in length • Too short • ↑chance of accidental decannulation • Too long • May abrade carina or rest in right mainstem • Longer tubes desirable if tracheal stenosis or malacia • Length confirmed by CXR or flex. endoscopy
Trach Tube Size Guidelines Diameter • Too large • Mucosal injury, stenosis • Inability to voice • Too small • Excessive leak in ventilated pts • Inadequate air exchange • Difficult to suction adequately • Pedi trach tubes sized based on inner diameter, correspond to endotracheal tube sizes
Trach Tube Size Guidelines Child’s Age Inner Diameter (mm)
Shiley Pediatric Trach Tubes Options: Neo, Pedi, Pedi-Long (PDL), Pedi c Cuff (PDC), Pedi-Long c Cuff (PLC)
Bivona Trachs • Similar sizing • Neo and Pedi • Cuffed Tubes: TTS (tight to shaft) • Excellent option for pts who need cuff
Bivona FlexTend Trach Tubes Flexible extended length connection ‘built-in’ to trach
Decannulation • Suitability: • Off ventilator, minimal suctioning requirement, no obstructive pathology • Tolerates capping/occlusion • Recent bronchoscopy is clear • Procedure: • Admission to ICU, monitoring • Downsizing vs removal, occlusive dressing • Observation 24-72 hrs