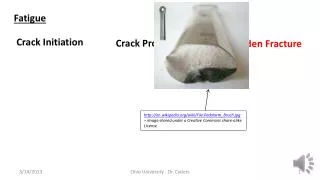
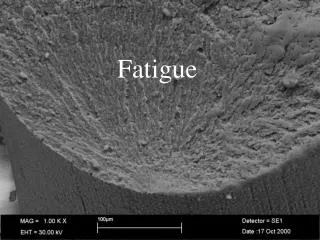
Fatigue
Fatigue. Implications for the Medical Profession Eleanor M. Duduch M.D. Program Director Anesthesiology Residency Program University of Massachusetts Medical School. Why So Much Concern in Medicine About Being Sleepy?. Significant increase in sleep research and

Fatigue
E N D
Presentation Transcript
Fatigue Implications for the Medical Profession Eleanor M. Duduch M.D. Program Director Anesthesiology Residency Program University of Massachusetts Medical School
Why So Much Concern in Medicine About Being Sleepy? • Significant increase in sleep research and outcome studies in recent years • Negative outcomes secondary to fatigue are so well documented that industry has led the way in developing sleep regulations - Military - Maritime - Trucking - Aviation • Where’s Medicine?
History of the Problem • 1986 Libby Zion vs. New York State • 18 yr. old with recent hx cocaine and MAOI use • admitted to New York Hospital with agitation and temp 103 • medical team consisted of a PGY-1 (18 hrs awake) & PGY-2 (19 hrs. awake), with little attending involvement • rigors treated with 25 mg. Demerol • died next a.m. with seizures and temp 108 • 11 year trial, split verdict (cocaine & negligence both factors) • Jury claimed fatigue, inexperience and lack of supervision as contributing factors toward claim of negligence
……Rapid Response….. • 1987 Bell Commission • A blue ribbon panel responsible for work hour recommendations in New York that eventually became the “405 Regulation” • 1989 NY State 405 regulation instituted • Largely ignored for first 10 years; financial penalties instituted and ignored as well • 1999 Institute of Medicine published a patient safety report “To Err Is Human: Building a Safer Health System”, revealing that medical errors contribute to many hospital deaths and adverse events • 2000 Presidential Task Force developed to address the issue
….Rapid Response… • 2001 OSHA was petitioned by Public Citizen group to implement new regulations on resident work hours • This brought the issue to national prominence • 2001 Patient and Physician Safety and Protection Act HR3236 was introduced in Congress • 2002 ACGME quickly proposed their own standards • 2003 Standards approved • July 1, 2003 Compliance required
ACGME STANDARDS • 80 hours maximum/week • 24 hours max per shift; add’l 6 hours for education and transfer of care • 1 day in 7 free of patient care responsibilities • In-house call q 3 nights averaged • 10 hour minimum rest period
ACGME STANDARDS • In order to provide high quality education & effective patient care, residency programs must: • Recognize & monitor residents for signs of fatigue • Apply preventive & operational countermeasures • Make clinical assignments that recognize a collective responsibility to patient care
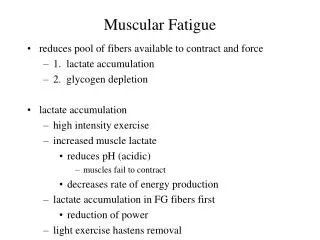
The Extent of the Problem • 2002 Multi-center Survey of Medical Residents vs. Patients @ Cleveland VA Sleep Disorders Clinic • Self-reporting surveyre: likelihood of dozing • Results recorded on Epworth Sleepiness Scale • 8 items, scored 0-3 scale, with 24 as highest possible score • Results: Sleepiness in residents is equivalent to that found in patients with serious sleep disorders
American Academy of Sleep Medicine Epworth Sleepiness Scale Sleepiness in residents is equivalent to that found in patients with serious sleep disorders. Mustafa and Strohl, unpublished data. Papp, 2002 © American Academy of Sleep Medicine
The Potential Impact of Sleep Loss & Fatigue Is Underestimated • In general there is a lack of knowledge about the biology of sleep, particularly by physicians • Signs of sleepiness are often unrecognized by the individuals or observers • There is no drug test to evaluate fatigue level • The culture of medicine • “sleep is optional (and you’re a wimp if you need it)” • “less sleep = more dedication”
MYTHS ABOUT FATIGUE • FALSE: “As long as I’m awake, I’m OK to work” TRUE: Being “awake” does not mean that your cognitive performance, judgment or reaction time is not affected by lack of sleep. Performance starts to decline after 15-16 hours of continued alertness. • FALSE: “I’m still OK to drive home after 24…30 hours on call” TRUE: The period of most limited attention span after being awake for 24 hours is between 6 a.m. and 11 a.m. • FALSE: “I can learn to get by on less sleep” TRUE: You cannot change how much sleep you need. It is a physiologic need, genetically determined • FALSE: “A good nights’ sleep and I’ll be fine” TRUE: Recovery of sleep debt developed over a 24 hour call period without sleep can take 2 full nights’ sleep to get back to baseline • FALSE “I can tell when I’m too tired to work” TRUE: Many studies have shown that individuals have little insight into their level of sleepiness. The more tired you are, the less accurate is your perception of how sleepy you really are!
Anesthesia Resident Study • Daytime sleepiness was assessed in 11 residents using the Multiple Sleep Latency Test • Daytime sleepiness was assessed in the baseline, post-24 hour call, and extended sleep (they were allowed to sleep as long as they needed x 4 days) conditions via polysomnography, EEG, EMG,EOG • Results: Residents’ daytime sleepiness in base-line and post-call conditions was near or below levels associated with sleep disorders. Extending sleep time resulted in normal levels of sleepiness. • Residents did not perceive themselves to be asleep 49% of the time there was physiologic sleep identified by EEG • Residents were wrong 76% of the time when they reported having stayed awake Howard et al, Acad Med 2002; 77(10):1019-1025
SO HOW DO I KNOW WHEN I’M NOT GETTING ENOUGH SLEEP?? • You and/or others notice your work performance is not up to your previous standards • You find yourself “nodding off” to sleep during lectures, breaks, lunch etc. • You become less efficient in your work routine, taking longer to accomplish the same tasks • You have trouble focusing • It is difficult to become motivated • You became more impatient with patients, friends, family members and colleagues
Wakefulness and Sleep The key determinant that underlies fatigue is the interaction of sleep homeostasis and circadian rhythm • Homeostatic sleep drive • regulates the length and depth of sleep • Endogenous circadian rhythms • influence timing and duration of daily sleep/wake cycles • Influence of external and internal stimuli • Workload, stress, boredom, motivation, environment all effect sleep. It is important to note that environmental factors can unmask fatigue (a warm/dark room, boring lecture, uninteresting topic), but do not cause sleepiness. • Optimal performance = adequate sleep + circadian wakefulness
In Other Words…..Sleep Is Not Negotiable!It is a physiologic drive…….
Q. What is “Adequate” Sleep? Balance between sleep quantity and sleep quality
HOW MUCH SLEEP IS ENOUGH?? MYTH “I’m one of those people who don’t need much sleep” FACTS • Avg. sleep need for optimal performance is 8hrs.14min • Individual variance is from 6-10 hours • Individuals have varying tolerance to effects of sleep loss….BUT self-assessment of sleepiness has been proven to be inaccurate • Acute sleep deprivation: 0-4 hrs sleep in 24 hours • Chronic sleep deprivation: repetitive sleep cycles of <7-8 hrs./day. • <5 hrs of sleep increases sleep drive and propensity to sleep, with associated decline in cognitive performance. • Creation of “sleep debt”
SLEEP DEBT • Definition: The accumulation of ‘lost sleep’ • ‘Lost sleep’ averages 1-1.5hrs/night for most individuals • Sleep debt is not repaid hour for hour • Example: 1.5 hrs. less sleep/night x 5 nights= 7.5 hrs. of sleep debt requiring (2) 8hr sleep periods
WHAT MAKES A GOOD NIGHT’S SLEEP?? • Non-REM sleep (75-80%) (low brain activity) • Stage 1 @ sleep-wake transition “light” • Stage 2 “true” sleep • Stages 3 & 4 “deep” or “delta” sleep • Highest arousal threshold-most difficult to awaken • Most restorative • REM sleep (20-25%;4-6 episodes/night) • Nearly absent muscle tone except respiration • High levels of cortical activity- dreaming, irregular respiratory and heart rates
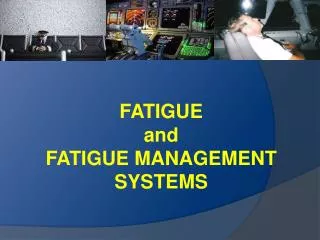
FRAGMENTED SLEEP • Interferes with a good night’s sleep • Most common in those age > 50 years • Sleep Disorders • Obstructive sleep apnea • Restless leg syndrome • Insomnia • Learned/conditioned • Medication induced • Alcohol • REM suppressant first half of night • Rebound REM as ETOH concentration decreases, with increased awakenings & decrease in total sleep time • External stimuli – pagers, phone call, anticipation, etc.
American Academy of Sleep Medicine Sleep Fragmentation NORMAL SLEEP = Paged MORNING ROUNDS ON CALL SLEEP © American Academy of Sleep Medicine
The Circadian Factor • Suprachiasmatic nucleus (SCN) of hypothalamus • Sets the biological clock to 24.18 hours • Easier to stay up late than go to sleep early • Controls body temperature cycles ↑ during day, ↓ at night • Uses light as synchronizer via retino-hypothalamic pathway • Melatonin as complementary synchronizer of SCN • Secreted at night by pineal gland • Suppressed by light • Controls physiologic, behavioral & mood functions • 24 hr. sleep-wake pattern • Daily digestive activity, BP changes, renal function • Hormone secretion – prolactin, testosterone, GH
The Circadian Factor • Circadian nadir • Lowest levels of alertness, activity & performance • Greatest vulnerability to errors and accidents • Increased sleepiness from 3-6 a.m. and 2-5 p.m. • Peak in fatigue-related MVA between 6-9 a.m. • Circadian peak • Maximal alertness from 9-11 a.m. and 9-11 p.m.
CONSEQUENCES OF SLEEP DEPRIVATION • Safety Issues • Performance Issues • Medical Errors • Health Correlates • Medical Education • Professionalism • Personal and Family Life
…..Consequences • Skills that are especially vulnerable to fatigue and sleep loss are uniquely human: • Motivation • Creativity • Judgment • Decision-making • Interpersonal happiness
Safety Risks of Fatigue SOCIETAL • Three Mile Island and Chernobyl nuclear accidents • Circadian factors • NASA Challenger • Flawed decision making from poor work-rest patterns of managers • Exxon Valdez marine grounding • Alcohol and fatigue PERSONAL • Increase in blood-borne pathogen exposure incidents • Risk is 50% greater at night • Motor vehicle collisions: 100,000 crashes, 76,000 injuries & 1,550 fatalities annually • NTSB 2001 poll “1:2 drivers report driving while drowsy; 1:5 report “nodding off” while driving”
4 SECONDS CAN END YOUR LIFE All it takes is a brief 4 second break in your attention to cause a fatigue related crash
RECOGNIZE THE SIGNS OF DROWSY DRIVING • Getting home and not remembering driving past the usual landmarks i.e. not remembering driving the last few miles • Difficulty focusing on road • Wanting to “rest your eyes” for just a second or two • Drifting across lanes • Missing exits • Closing your eyes whenever you have a chance i.e. at stoplights, crosswalks etc. • Be aware of microsleep
MICROSLEEP • Brief, uncontrolled and spontaneous episodes of physiologic sleep • Significant performance reductions sufficient to create safety risks before & after a microsleep • Usually no subjective awareness
FATIGUE RELATED CRASHES • <5 hours sleep increases risk of involvement in sleep-related vs. non sleep-related crash by 4.5 times • Greater likelihood of serious injury • Usually a single occupant off-road accident • Risk increases with certain conditions • Alcohol - it doesn’t have to be a lot! • Medical conditions including sleep apnea • Medications • Solo driving • Driving for long stretches or along roads with little visual stimulus • Often dependent on time of day – most occur between 6 a.m. and 9 a.m.
DROWSY DRIVING: WHAT DOESN’T WORK!! • Turning up the radio • Opening the car window and letting the cold air blow on your face • Singing/talking to yourself • Eating/chewing gum/drinking fluids
DROWSY DRIVING: WHAT DOES WORK • If you are really tired, don’t try to drive home. Thinking “it’s just a short drive…I’m fine” is dangerous. Get someone to drive you home, take a taxicab or a bus. • Take a nap before driving home. Although a short 30 minute snooze will help, a 2 hour nap is best (allow sleep inertia to pass before getting into a car) • If you notice any of the warning signs of drowsiness, don’t ignore them. Get off the highway/road, pull into a safe area (parking lot etc.), lock your car and take a nap.
Automobile Accidents and EM Residents & Faculty • Prevalence rates for: • Collisions up to 8% (74% post night shift) • Near misses up to 58% (80% post night shift) • Correlated with: • # of night shifts worked • Resident’s self-reported tolerance of shift work • Self-reported adaptation to drowsiness Steele MT, The occupational risk of motor vehicle collisions for emergency medicine residents. Acad Emer Med 1999;6:1050
Automobile Accidents and Pediatric Residents & Faculty • Prevalence Rates for: • Falling asleep at the wheel: • Residents 49% • Faculty 13% • Motor Vehicle Accidents • Residents 20 • Faculty 11 • Traffic citations • Residents 25% • Faculty 18% Marcus CL. Effects of sleep deprivation on driving safety in house staff. Sleep 1996, 19:763
PERFORMANCE ISSUES • Reduced vigilance, impaired memory & decision-making, prolonged reaction time • Increased risk for errors and critical incidents • Increased performance variability – consistency in knowledge, judgment and actions diminishes • Speed-accuracy trade-off i.e. in order to maintain same level of accuracy in decision-making, it takes more time to think through the situation • Impairment from 24 hr. sustained wakefulness is equivalent to 0.1% blood alcohol level
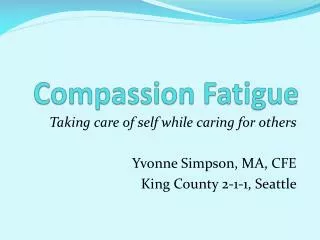
Effects of Sleep Deprivation on Functioning Dawson D, Reid K. Fatigue, alcohol and performance impairment. Nature 1997;388(6639):235.
Effects of Sleep Deprivation on Functioning Dawson D, Reid K. Fatigue, alcohol and performance impairment. Nature 1997;388(6639):235.
IMPACT ON PERFORMANCE • Surgery • 24% more errors & 14% more time to perform simulated laparoscopy post-call Taffinder et al, Lancet.1998; 352 • 2-fold increase in errors & 38% increase in time required for same task Grantcharov et al, BMJ. 2001; 323 • Internal Medicine • Efficiency & accuracy on simulated ECG interpretation deteriorated Lingenfelser et al, Med Educ. 1994; 28 • Pediatrics • Efficiency on task performances decreased significantly at 24 hours of wakefulness Storer et al, Acad Medicine; 64
MEDICAL ERRORS • Surveys: 60% U.S. anesthesiologists & 90 % Australian anesthesiologists report making fatigue-related errors Gravenstein et al, Anes. 1990;72 Gander et al,Anaesth Intensive Care 2000;28 • IM residents- 41% their “most significant medical mistake” was secondary to fatigueWu et al, JAMA 1991;265(16) • Case reviews of fatigue-related complications: • 3% of 5600 reported anesthesia incidents/10 years Morris et al, Anaesth Intensive Care2000;28 • 5% of “preventable incidents” & 10% of drug errors Williamson et al, Anaesth Intensive Care 1993;21 • Post-op surgical complication rates 45% higher when resident post-call Haynes et al,S.Med J. 1995
American Academy of Sleep Medicine Work Hours, Medical Errors, and Workplace Conflicts by Average Daily Hours of Sleep* *Baldwin and Daugherty, 1998-9 Survey of 3604 PGY1,2 Residents © American Academy of Sleep Medicine
HEALTH CORRELATES • Physiologic alterations • Depression of immune function • CHO metabolism & endocrine dysfunction • Abnormal glucose tolerance • Decreased thyrotropin concentrations • Increased SNS activity • Cerebral metabolic & cognitive function • Decreased CMR in thalamus, frontal & parietal cortices • Adverse pregnancy outcomes • Independent risk factor for CV and GI disease
American Academy of Sleep Medicine Adverse Health Consequences by Average Daily Hours of Sleep* *Baldwin and Daugherty, 1998-9 Survey of 3604 PGY1,2 Residents © American Academy of Sleep Medicine
IMPACT ON PROFESSIONALISM • Negative change in attitude toward patients • Conflicts with staff and colleagues • Loss of empathy/compassion • Role resistance • Resentment and disenchantment with profession
Negative Effects of Sleep Deprivation on Professionalism Decreased Motivation: “I keep thinking he’s blue enough to go the ICU. I keep hoping he’s too blue to go anywhere. Probably a nice man with a loving wife and concerned children, but I don’t want the SOB to make it because I’ve got one patient who is going to keep me up two more hours…I don’t want the asthmatic SOB to live if it means I don’t sleep. I don’t want the patient to live if it means I don’t sleep. I just want to sleep.”1 1.Excerpt from trainee diary: L C Groopman. Medical internship as moral education: an essay on the system of training physicians. Cult Med Psychiatry 1987; 11: 207–27.
IMPACT ON PERSONAL AND FAMILY LIFE • Mood disturbances • Increased stress/anxiety • Potential for alcohol and substance abuse • Negative effect on motivation
HOW TO STAY ALERT • Naps • CNS Stimulants • Caffeine • Medications • Melatonin • Better scheduling • Sleep!
NAPS Temporarily improve alertness but do not replace a good night’s sleep!! • Types • Preventative (pre-call) • Operational (on the job) • Length • Short naps < 30 min. helps avoid grogginess known as “sleep inertia” • Long naps 30-240 min. • Timing • Take advantage of circadian windows (2-5 am & 2-5 pm)
SLEEP INERTIA WHAT IS IT? • Grogginess or incomplete arousal from sleep • Most likely to occur after 3-4 hours sleep WHAT ARE ITS EFFECTS? • Slowed speech • Poor memory • Performance deficits • Impaired decision making • May take up to 1 hour to clear