Download
1 / 14
140 likes | 259 Views
SBIRT: Addressing unhealthy substance use in primary care. Christine Pace, MD, MSc Assistant Professor of Medicine, Boston University School of Medicine Lee Ellenberg , LICSW Training Manager, MASBIRT Training and Technical Assistance (TTA) April 3, 2014. Outline. Outline.

E N D
SBIRT: Addressing unhealthy substance use in primary care Christine Pace, MD, MSc Assistant Professor of Medicine, Boston University School of Medicine Lee Ellenberg, LICSW Training Manager, MASBIRT Training and Technical Assistance (TTA) April 3, 2014
Outline Outline • Impact and spectrum of unhealthy substance use in primary care • Screening, brief intervention and referral to treatment (SBIRT) • Approach • Effectiveness • Implementation opportunities & resources
Unhealthy substance use in primary care • Spectrum of use that risks health consequences • Cardiovascular disease, cancer, trauma, infection, more • Alcohol = 3rd leading preventable cause of death in US1 • Costly: • Societal costs of $416.5 billion annually2 • Underdiagnosed • 16% of patients ever discussed alcohol with provider3 • Undertreated • 14% with substance use disorders (SUD) in MA get treatment4 1 http://www.prevent.org/National-Commission-on-Prevention-Priorities/Rankings-of-Preventive-Services-for-the-US-Population.aspx ;2 Bouchery, Am J Prev Med 2011:41;516-524; 3. CDC Vital Signs Report 2013 http://www.cdc.gov/vitalsigns/ ; 4. Brolin, MA Health Policy Forum 2005
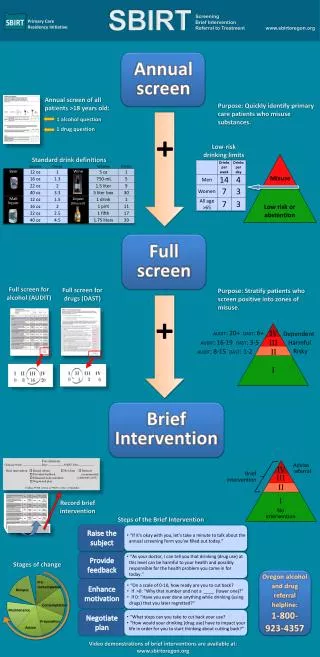
Addiction:HistoricalPerspective New concept Risky use Unhealthy use • Risky use: • For alcohol— • Men < 65: >4 drinks/occasion or >14 drinks/wk • Women & >65: >3 drinks/occasion or >7 drinks/wk • For drugs*--ANY use SUD Problem No Problem Low risk use or no use http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/guide.pdf
What is SBIRT? • A low intensity, low cost, public health approach to identify and intervene with people with unhealthy substance use. • Screening:Universal, brief questionnaire that identifies unhealthy substance use • If positive: Additional questions to determine severity and consequences of use • Brief Intervention:Brief conversation to raise awareness of risks & build motivation to change • Referral to Treatment:For those with more serious problems, when appropriate
Why is SBIRT important? • Patients often don’t understand impact of alcohol and drug use on health • Particularly unaware of drinking guidelines • Clinician suspicion of alcohol problems has poor sensitivity (27%) for identifying patients with (+) screen for unhealthy alcohol use1 • Lack of confidence in substance use assessment and intervention is associated with lower MD satisfaction in working with patients with SUD2 1 Vinson, D, Annals of Fam Med. 2013; 2 Saitz, R, J Gen Intern Med. 2002.
The key to SBIRT: Brief intervention ….a brief, non-judgmental, non-confrontational, directive conversation, using Motivational Interviewing (MI) principles & techniques to enhance a patients’ motivation to change their use of alcohol and other drugs.
Brief intervention Brief intervention • Feedback: provide personalized feedback based on screening results; state concern regarding medical risks/consequences of use • Advice: ask permission; then, make explicit recommendation for change in behavior; discuss patient’s reaction • Seal the Deal: enhance motivation for behavior change; elicit ideas &negotiate plan with patient, schedule follow-up
SBIRT effectiveness SBIRT has been found to: Help patients reduce alcohol use1,2, Increase proportion with SUD who get treatment3 Reduce healthcare costs4,5: Alcohol SBI in primary care reduces ED visits and inpatient days, and saves $3 for every healthcare dollar spent.6 Most effective for lower severityalcohol use in primary care7,8 Ongoing research: Drugs, other settings & severities, teens USPSTF recommends alcohol SBI (grade B) Why is SBIRT important? 1 Babor, T Sub Abuse 2007; 2 Mertens, J Alc Clin Exp Res 2005; 3 Krupski, A Drug Alc Dep 2010; 4 Solberg, L, Am J Prev Med, 2008; 5 Estee, S Medical Care 2010; 6 Fleming, M, Medical Care. 2000; 7 Kaner, E Drug Alc Review 2009; 8 Saitz, R Ann Intern Med 2007; USPSTF=US Preventive Services Task Force
Rankings of 25 Preventive Services Recommended by USPSTF • Ranked higher than: • Screening for high BP or cholesterol • Screening for breast, cervical, or colon cancer • Adult flu, pneumonia, or tetanus immunization Maciosek, Am J Prev Med, 2006; Solberg, Am J Prev Med 2008; http://www.prevent.org/content/view/43/71 1 = lowest; 5 = highest 10 Adapted from Partners in Integrated Care
Implementing SBIRT: Challenges and opportunities SBIRT implementation challenges & opportunities Challenges Opportunities New payment models Team-based care Broad-based behavioral health integration efforts (enhance training opportunities, access) • Limited reimbursement • Workflow challenges • Training gaps • Poor access to specialty substance use treatment
SBIRT in action: BMC Primary Care • Front desk: Gives screen to patient • Single-item alcohol and drug questions • PHQ-2 for depression • Medical assistant: Scores screen, gives follow-up tool for any (+) response • AUDIT, DAST-10 and/or or PHQ-9 • Provider: Scores any follow-up tool; as needed, conducts BI and/or places referral.
MASBIRT Training & Technical Assistance (TTA) (www.masbirt.org) Supported by MA DPH: Bureau of Substance Abuse Services (BSAS) to build statewide SBIRT awareness and capacity to • implement and integrate SBIRT into diverse settings and organizations, • and promote clinician SBIRT skills and competency. www.maclearinghouse.com
Conclusions Conclusions • SBIRT is an evidence-based, cost-saving intervention to reduce unhealthy substance use among primary care patients • SBIRT training and implementation should emphasize brief intervention • Healthcare reform and behavioral health integration efforts present opportunities for broad implementation of SBIRT • MASBIRT TTA is a resource to support implementation (www.masbirt.org)