Download
1 / 25
470 likes | 1.66k Views
Fever of Unknown Origin. AIMGP Seminar Series Dr. Katina Tzanetos February 2007. References. Mourad, O., et al. A Comprehensive Evidenced-Based Approach to Fever of Unknown Origin. Arch Inter Med 163: March 10, 2003.

E N D
Fever of Unknown Origin AIMGP Seminar Series Dr. Katina Tzanetos February 2007
References • Mourad, O., et al. A Comprehensive Evidenced-Based Approach to Fever of Unknown Origin. Arch Inter Med 163: March 10, 2003. • Roth, A. and Basello, G. Approach to the Adult Patient with Fever of Unknown Origin. American Family Physician 68 (11), 2223. • Up To Date. • Approach to the adult with fever of unknown origin • Etiologies of fever of unknown origin in adults * Much of this talk based on very helpful article by Mourad et al. – Highly recommended
Case Discussion – Based on Real Patient • 28-year old female, born in Canada, parents from Hong Kong • 2.5 week history of fever 40.0C or higher • Only other symptom is possible rash on lower legs – intermittent, tender, red nodules • Works in bank • Non-smoker, non-drinker • Only medication is OCP
Take a minute to discuss… • Does she fit the criteria for Fever of Unknown Origin • Why or why not?
Fever of Unknown Origin - Definition • Classic definition • Temperature higher than 38.3C • Several occasions • Cause obscure after 1-week of in-patient evaluation • Current definition • recognizes acceptability of out-patient in place of in-patient investigations
Case Discussion • Based on short duration and absence of investigations patient does not fit diagnostic criteria • If fever persists, should pursue diagnosis • Her fever persists • What aspects of the history and physical examination do you focus on during this initial visit?
Four Proposed Categories of FUO • Based on potential etiology of FUO • All require temperature > 38.3C • Categorization be especially helpful in organizing an “approach” to patient evaluation • Classic • Nosocomial • Immune-deficient (neutropenic) • HIV-related
Classic Category of FUO • Definition: • Duration > 3 weeks, evaluation of at least 3 outpatient visits or 3 days in-hospital • Common etiologies: • Infection, malignancy, CVD This category will be the focus of this talk
Nosocomial Category of FUO • Definition: • Hospitalization of at least 24 hrs with no fever on admission, evaluation of at least 3 days • Common etiologies: • C.Difficile, drugs, PE, septic thrombophlebitis, sinusitis (intubated patients)
Immune-deficient (neutropenic) Category of FUO • Definition: • Neutrophil count < 500/mm3, evaluation of at least 3 days • Etiologies: • Opportunistic bacterial infections, aspergillosis, candidiasis, herpes virus
HIV-Associated Category of FUO • Definition: • Duration of at least 4 weeks for outpatients and 3 days for inpatients, HIV confirmed • Etiologies: • Cytomegalovirus, MAI, Pneumocystis, drugs, Kaposi’s, lymphoma
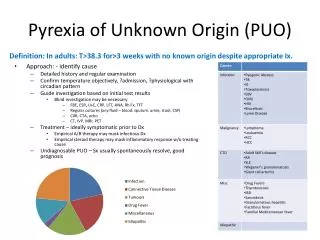
Etiology and Epidemiology of Classic FUO • Infections: Most common cause accounting for 1/3 of cases • TB; Most common infection in non-elderly adults • PPD positive in less than 50% of pts with TB and FUO, Sputum samples positive in only ¼ of patients • Abscesses • Usually in abdomen or pelvis with some pre-disposing cause (e.g. recent surgery, diabetes, biliary tract disease, recent UTI) • Other infections: Osteomyelitis, endocarditis (esp. in pts with recent antibiotic use or HACEK organisms) • Malignancy: Second most common cause • Lymphoma (esp. non-Hodgkin’s), Leukemia, Renal cell, HCC, other metastasis to liver • CVD: Third most common cause • Adult Still’s disease in younger patients and giant cell arteritis in older patients
Diagnostic Approach - History • History • Travel • Exposures to toxins, sick persons, animals • Immunosuppression • Localizing symptoms • Look for subtle findings: eg. Jaw claudication, nocturia with prostatitis • Degree of fever, nature of fever curve, apparent toxicity, and response to antipyretics not specific enough to guide management
Diagnostic Approach – Physical Examination • Repeated examination may be needed • Careful attention to skin, mucous membranes, lymph and abdominal system • Ask pts to record and measure temperature daily • Yield from history and physical examination unknown
Back to the case… • Thorough history and physical non-contributory except for intermittent skin lesions • Given what you know thus far, what investigations would you order?
Diagnostic Approach – Laboratory Investigations • Suggested minimal diagnostic work-up to qualify as FUO has varied over the years • Recent article by Mourad et al suggests following as minimal: • History and physical examination • CBC and differential • Blood film reviewed by hematopathologist • Routine chemistry including LDH, bilirubin, liver enzymes • Urinalysis and microscopy • ANA, RH factor • HIV • CMV IgM; heterophil test if suspicious for Mononucleosis • Q-fever serology (if risk exists) • CXR • Hepatitis serology (if abnormal liver enzymes)
Diagnostic Approach – Investigations and the Evidence • Abdominal CT • Useful to look for abdominal lymphoma and abscess • Diagnostic yield in case series 19% • Clinical follow-up showed that only 1/32 patients with normal scans had an intra-abdominal cause for FUO
Diagnostic Approach – Investigations and the Evidence • Nuclear Imaging: • For localizing inflammatory or infectious focus • Technetium scans likely have best test characteristics overall and should be test of choice • Technetium studies: specificity 93%, sensitivity 40-75%; PLR 5.7-12.5 • Indium-labeled WBC scans: specificity 69%-86%, sensitivity 45%-82% • Gallium scans: (limited studies)
Diagnostic Approach – Investigations and the Evidence • Duke criteria for endocarditis: • Endocardities: 1-5% of all cases of FUO • Sensitivity 82%, specificity 99% • Liver Biopsy: • Diagnostic yield 14%-17% regardless of whether abnormal physical exam or liver enzymes exist • Complications in FUO from biopsy only 0.32% at most • Recommended
Diagnostic Approach – Investigations and the Evidence • Temporal artery biopsy • Large studies comprised of elderly with FUO lacking • Arteritis cause of FUO ~16% of pts (All comers) • Safe, recommended in elderly with FUO • Leg dopplers • DVT cause of FUO ~ 2-6% of pts • Safe, easy to do, recommended
Diagnostic Approach –Investigations and the Evidence • Bone Marrow Examination • Diagnostic yield of culture 0-2% • Not recommended in immunocompetent pts • Abdominal exploration • Role of surgery in post-CT era uncertain • Empiric Therapy (antibiotics, anti-TB, steroids) • Not studied • Not recommended
Proposed Diagnostic Algorithm Mourad, O. et al. Arch Intern Med 2003;163:545-551.
Back to the case… • CBC and differential, electrolytes, BUN, creatinine, Ca/Mg/Ph all normal • Liver enzymes very slightly elevated then normalized (AST 68normal, ALT 78normal), bilirubin, ALP normal • Multiple blood cultures: no growth • ESR 39 • Hepatitis, Lyme, PPD, Mononucleosis, Q-fever, HIV serology all negative, ANA, RF negative • CT thorax and abdomen normal • 2D Echo normal • Leg dopplers negative • Skin biopsy: unremarkable epidermis and dermis, no subcutaneous material obtained; lesions resolved
Back to the case… • Fever of > 40C continued for more than 4 weeks • No diagnosis despite multiple out-pt visits and a short in-hospital stay • Debated about going to bone marrow biopsy versus liver biopsy • Decided on nuclear scan • However, pt was given short course of oral antibiotics by family MD, symptoms resolved, pt cancelled all further tests and follow-up appointments with us and is doing fine
Conclusions from Case • Given our modern-day advances, prognosis in patients who truly have no diagnosis after extensive recommended work-up is very good (most sinister diagnoses are discovered) • In some cases, spontaneous resolution occurs, in others, watchful waiting is necessary (but often frustrating) • 1930s: > 30% of FUO with no diagnosis died • Today: 50-90% or more recover spontaneously