Download
1 / 27
460 likes | 1.26k Views
Fever of Unknown Origin. Definition. Fever > 38.3 on several occasions Fever lasting more than 3 weeks No diagnosis despite 1 week of inpatient workup. Potential Etiologies. Based on patient population Classical Immunodeficient (Neutropenic) Nosocomial HIV related. Classic FUO.

E N D
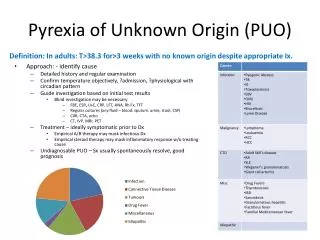
Definition • Fever > 38.3 on several occasions • Fever lasting more than 3 weeks • No diagnosis despite 1 week of inpatient workup
Potential Etiologies • Based on patient population • Classical • Immunodeficient (Neutropenic) • Nosocomial • HIV related
Classic FUO • Fever > 38.3 • Duration greater than 3 weeks • Evaluation for 3 weeks as an outpatient or 3 days in hospital
Classic FUO • Infection • Malignancy • Collagen vascular diseases
Nosocomial FUO • Fever > 38.3 • Patient hospitalized > 24 hours, but no fever on admission • Evaluation for at least 3 days
Nosocomial FUO • Clostridium difficile • Drug induced • Pulmonary embolism • Septic thrombophlebitis • Sinusitis
Neutropenic FUO • Fever > 38.3 • ANC 500 or less • Evaluation for at least 3 days
Neutropenic FUO • Opportunistic bacterial infections • Herpes Virus • Aspergillosis • Candidiasis
HIV FUO • Fever > 38.3 • Duration > 4 weeks (outpatient) or > 3 days (inpatient) • HIV infection confirmed
HIV FUO • CMV • MAC • PCP • Drug induced • Kaposi’s Sarcoma • Lymphoma
Infections • Tuberculosis (especially extrapulmonary)Abdominal abscessesPelvic abscessesDental abscessesEndocarditisOsteomyelitisSinusitisCytomegalovirusEpstein-Barr virusHuman immunodeficiency virusLyme diseaseProstatitisSinusitis
Infections • As duration of fever increases, infectious etiology decreases • Malignancy and factitious fevers are more common in patients with prolonged FUO.
Malignancies • Chronic leukemiaLymphomaMetastatic cancersRenal cell carcinomaColon carcinomaHepatomaMyelodysplastic syndromesPancreatic carcinomaSarcomas
Autoimmune • Adult Still's diseasePolymyalgia rheumaticaTemporal arteritisRheumatoid arthritisRheumatoid feverInflammatory bowel diseaseReiter's syndromeSystemic lupus erythematosusVasculitides
Miscellaneous • Drug-induced feverComplications from cirrhosisFactitious feverHepatitis (alcoholic, granulomatous, or lupoid)Deep venous thrombosisSarcoidosis
Diagnosis • Failure to reach a diagnosis is not uncommon • 20% of cases remain undiagnosed • Even if extensive investigation does not identify a cause, these patient’s still have favorable outcomes.
Diagnosis • Comprehensive History • Physical Exam • Confirm fever and document pattern • Laboratory Data
History • Recent travel • Exposure to pets and other animals • Sexual history • Work environment • Contact with other people with similar symptoms • Family history • Past medical history list of medications • Include OTC
Physical Exam • Skin • Mucus membranes • Lymphadenopathy • Organomegaly
Diagnosis • A cost-effective individualized approach is essential in the evaluation of these patients to prevent performing inappropriate tests.
Diagnostic Testing • CBC • LFTs • ESR • Urinalysis • Blood cultures • Further testing should be based on abnormalities in the initial workup
Diagnosis • PPD testing is inexpensive screening tool that should be used on all FUO patients that do not have a known positive reaction
Diagnosis • If initial testing is inconclusive- more specific testing should be performed based on clinical suspicion • Serologies • CT • Ultrasounds • MRI • Nuclear Medicine Scans
Chest radiograph Tuberculosis, malignancy, Pneumocystis carinii pneumonia CT of abdomen or pelvis with contrast agent Abscess, malignancy Gallium 67 scan Infection, malignancy Indium-labeled leukocytes Occult septicemia Technetium Tc 99m Acute infection and inflammation of bones and soft tissue MRI of brain Malignancy, autoimmune conditions PET scan Malignancy, inflammation Transthoracic or transesophageal echocardiography Bacterial endocarditis Venous Doppler study Venous thrombosis
Diagnosis • More invasive testing, such as LP or biopsy of bone marrow, liver, or lymph nodes, should be performed only when clinical suspicion shows that these tests are indicated or when the source of the fever remains unidentified after extensive evaluation. • When the definitive diagnosis remains elusive and the complexity of the case increases, an infectious disease, rheumatology, or oncology consultation may be helpful.