Download

1 / 19
220 likes | 525 Views
Adaptive support for patient-cooperative gait rehabilitation with the Lokomat. Duschau-Wicke, A; Brunsch, T; Lünenburger, L; Riener, R. Gait Rehabilitation. Walking disabilities stroke, spinal cord injury, traumatic brain injury, cerebral palsy , multiple sclerosis.

E N D
Adaptive support for patient-cooperative gait rehabilitation withthe Lokomat Duschau-Wicke, A; Brunsch, T; Lünenburger, L; Riener, R
Gait Rehabilitation • Walking disabilities • stroke, • spinal cord injury, • traumaticbrain injury, • cerebral palsy, • multiple sclerosis. • Body weight supported treadmill training • Shown to be effective especially in stroke.
Rehabilitation Procedures • Originally, these devices moved along predefined, fixedtrajectories, and they did not adapt their movements tothe activity (or passivity) of the patient. • early phase of rehabilitation or who are severely affected • Patients can remain completely passive, which leads to reduced activity of muscles and metabolism
Patient-Cooperativity • To improve these shortcomings, patient-cooperative controlstrategies are being developed by several research groups • Patient oriented movement with guidance and support • First efforts towards patient-cooperativity concentrated onthe addition of compliance to the devices • Impedance controller • Built-in compliance in design
Assist as Needed • To stimulate a maximum of voluntary contribution of the patient during treadmill training,robotic devices are supposed to reduce their supportive actions to a minimum. • This minimal support needs to besufficient to ensure that patients can complete the desired taskin a physiologically correct way • adjusting the stiffness and damping constants of a closed-loop impedance control
AIM • A different kind of adaptive support • The control parameters of the closed-loop controller are held constant – same compliance for the patient • An iterative learning controller to shape a supportive torque field along the movement trajectory • The support depends on the patient’s performance during the previous steps • provide individualized help in performing the desired movements while patientcan still move as freely as intended
Questions • Evaluated the adaptive support in an experiment with 3 healthy subjects. • Does the support adapt to the general activity (or passivity) of the subjects? • Doesthe resulting level of support reflect the individual needs ofthe subjects? • Does the support improve the performance of the subjects? • Proof-of-concept : algorithm iscapable of automatically adapting a supportive interventionto the degree of activity of a human subject.
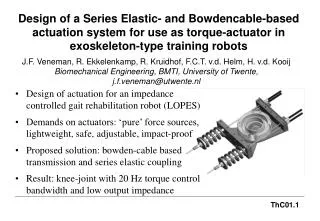
Device • Automatebody weight supported treadmill training of patients • 2actuated leg orthoses that are attached to the patient’s legs • one linear drive in thehip joint and one in the knee joint • Knee and hip joint torques from sensors • closed-loop controlled body weight support system
Controller • The Lokomat is controlled by an impedance controller • K can be influenced by the therapist. • B is chosen for critical damping • Tsup can be a deliberate, time-varying support profile -determined by the learning algorithm
Adaptive Support • An adaptation algorithm based on iterative learning control (ILC) to adjust Tsup. • The basic idea of ILC is the iterative improvement of aninput function for a cyclic process • Learning gain • Assist as needed adaptive controllers with a forgetting factor keep patients challanged
Error Definition • additional supportive torques during stance phase to prevent knee buckling without having to increase body weight support. • A dead zone of width d • Each cycle is defined to start with stance phase • The values of kf and kl were determined in iterative tests by trial and error
Experiment Conditions • 3 different Groups
Experiment Design • Under each condition, 3 Phases • For phase A1 and A2 : actively extend their knees during stance phase • For phase P : simulate not being able to carry theirbody weight
Data Processing • For each condition, the average support and the average controlerror during each stride (until swing phase) • The amount of support during phase P of conditions C1and C2 was compared if the support was adapted to individual needs • To study the effect of the adaptive support on the controlerror, condition C1 and condition C3 were compared
Results S1 S3 S2 • Averagesupport during stance phase for each step i • no significant difference between the active phases Passive Active
Results S1 S3 S2 • In all subjects, the support during passive walking with50% body weight support was significantly higher thanduring walking with 70% body weight support • If no support was provided (condition C3), the resultingcontrol errors during passive walking were significantlyhigher than for supported walking Passive Active
Discussion Key-Points • The support was adapted to different levels for differentsubjects, indicating that the subjects put the instruction towalk passively not equally well into practice • To test if the resulting support reflected the individualneeds of a subject, conditions with differentamounts of body weight support compared. • Artificially altered the need for support by taking away more or less bodyweight of our subjects via the harness attached to their trunk
Discussion Key-Points • Did support improved the performance of our subjects? • performance control error in theknee joints of the Lokomat • When the subjects walked passively, they did not stabilize their knees during stancephase and caused excess flexion also in the knee joints of the Lokomat. • Measuredin terms of thecontrol error, ↓error == an ↑ performance • However, the control error was notreduced to the (baseline) level of active walking • A residual error remained, which depends on the configurationof the forgetting factor kf , the learning gain kl, and the widthof the dead zone d. • more “supportive” or more “demanding
Limitations • Did not address the robustness of the algorithm • The limited number of subjects only allows fora proof-of-concept. • However, results show that the algorithmhas all the intended properties. Further studies need toaddress if these properties are sufficient for improving theclinical application of the Lokomat robot