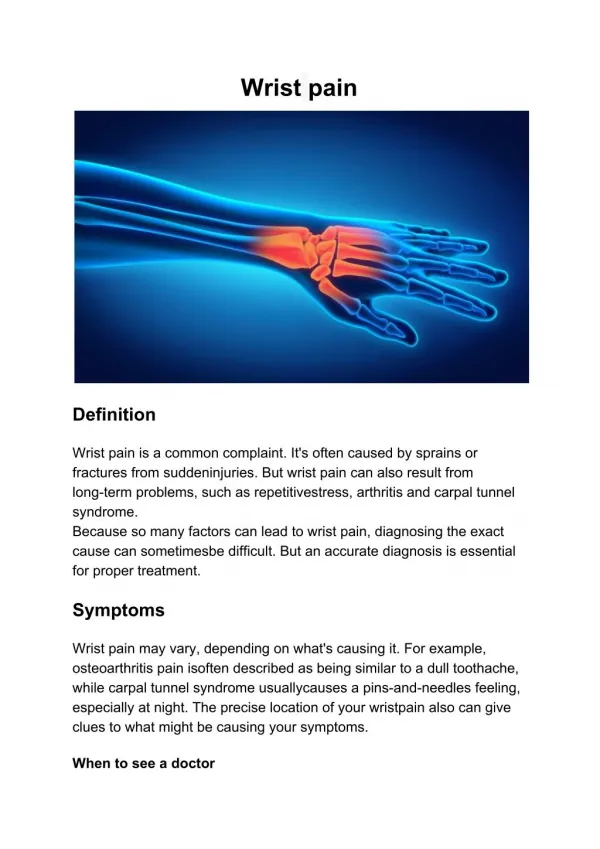
Normal wrist joint
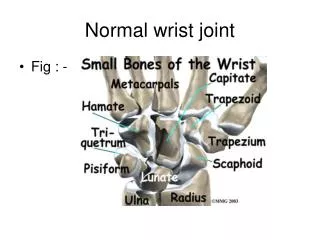
Normal wrist joint. Fig : - . Scaphoid fracture (skaphe=a boat, eidos=form). Features : 1 . This bone forms the radial part of the carpus. 2 . Articulates with 5 bones : - radius (proximally) , , Trapezoid and trapezium(distally) Lunate and capitate (medially )

Normal wrist joint
E N D
Presentation Transcript
Normal wrist joint • Fig : -
Scaphoid fracture (skaphe=a boat, eidos=form) Features : 1 . This bone forms the radial part of the carpus. 2 . Articulates with 5 bones : - • radius (proximally) , , • Trapezoid and trapezium(distally) • Lunate and capitate (medially ) 3 . Central indentation is called waist 4 . Since it crosses 2 rows of carpus , it is more susceptible to fracture 5 . Lies obliquely at 45 degree to longitudinal axes of 2 rows
Scaphoid fracture • Fig : - AP view
Scaphoid fracture • Fig : -
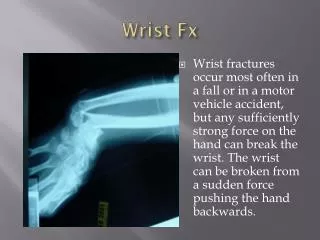
Aetiology • Common in young • Can be seen in patients of 10 – 70 years of age • Mechanism of injury Two different mechanisms • Compression injury : usually results in non displaced fx • Hyperextension bending injury : usually results in displaced fx
Diagnosis The diagnosis should be based on : History Clinical examination Radiographic evaluation
History • fall on an outstretched hand, athletic injury etc. • Common in young adult men • Pain at the radial side of the wrist • Associated injuries
Clinical Examination • tenderness in the anatomic snuff box • Tenderness to palpation over scaphoid tuberosity • Tenderness with axial compression of thumb toward the snuff box • Tenderness as patient supinates forearm against resistance
Anatomic snuff box Fig :
Clinical Examination • Radial & ulnar deviation results in pain on radial side of wrist • Forced dorsiflexion usually elicits significant tenderness • Limitation of wrist motion • Swelling – usually not present
Radiographic Evaluation • AP , • PA , • lateral, • scaphoid view ( PA with ulnar deviation )
Radiographic Evaluation • Motion views of the wrist ( flexion-extension-radial & ulnar deviation ) may demonstrate fracture displacement • If a diagnosis still can’t be confirmed (oblique views ) • If a diagnosis still can’t be confirmed (cast for 2 to 4 weeks and the clinical & radiographic evaluation repeated)
Radiographic Evaluation • If the second radiographic examination is still equivocal , a technetium bone scan, CT or MRI of the wrist is recommended • if the bone scan is negative , a scaphoid fx is ruled out • If the bone scan is positive, more specific studies ( e.g. CT or MRI ) can be helpful
DDx Lunate dislocation or fx Scapholunate instability Radial styloid fx Trapezium fx
Classifications of scaphoid fx • Anatomical classification :5 different fracture sites : 1 . Proximal third ( proximal pole ) .. 25% 2 . Middle third ( waist )… most common 65% 3 . Distal third …..10% 4 . Tuberosity 5 . Distal articular surface ( osteochondral fx )
Russe’s Classification : - • Direction of the fracture : - Horizontal Oblique , - Transverse , and - Vertical Oblique (unstable)
Cont.. • Time since injury : • Acute fracture - less than 3 weeks old • Delayed union - 4 to 6 months old • Nonunion - more than 6 months old
Classifications of scaphoid fx • Amount of fracture displacement ( stability ) : • Undisplaced ---- stable • Displaced ---- unstable
The unstable fracture (displaced) is defined as : - presence of a fracture gap > 1 mm on any radiographic projection - scapholunate angle > 60 - radiolunate angle > 15 - or intrascaphoid angle > 20
Scaphoid axis The true axis of the scaphoid is the line through the midpoints of its proximal and distal poles. Since the midpoint of the proximal pole is often difficult to appreciate, an almost parallel line can be used that is traced along the most ventral points of the proximal and distal poles of the bone (figure
Scapholunate angleNormal: 30 - 60°Questionably abnormal: 60 - 80°Abnormal: > 80° This indicates instability of the wrist. • Lunate axis: The axis of the lunate runs through the midpoints of the convex proximal and concave distal joint surfaces and can best be drawn by finding the perpendicular to a line joining the distal palmar and dorsal borders of the boneas demonstrated on the left Scapholunate angleNormal: 30 - 60°Questionably abnormal: 60 - 80°Abnormal: > 80° This indicates instability of the wrist.
Capitolunate angleNormal: < 30°Abnormal: > 30°.This indicates instability of the wrist Capitate axis • The capitate axis joins the midportion of the proximal convexity of the third metacarpal and that of the proximal surface of the capitate.Capitolunate angleNormal: < 30°Abnormal: > 30°.This indicates instability of the wrist
Treatment • Undisplaced ( stable) fracture : • Nonoperative ( cast immobilization )--- above elbow casts
a short arm thumb spica with the thumb interphalangeal joint free. The wrist is placed in radial deviation • Long arm cast is recommended for nondisplaced proximal pole fx
Time to healing by location : • Distal third fx heals in 6-8 weeks • Middle third fx 8-12 weeks • Proximal third fx 12-24 weeks
Removal of the cast should not occur until union has been documented on CT or tomography • Prognosis is excellent in undisplaced, stable fractures if diagnosed and immobilized early
Treatment • Displaced fractures : • Primary internal fixation (for unstable scaphoid fx ) • treated by primary internal fixation, average time for return to work is 3 – 4 weeks with union rate 97 %
Indications of Surgery in Scaphoid fractures - Displaced acute fracture - Delayed union or nonunion - S.Fx associated with a perilunate fx or dislocation - Ligamentous injury - Non displaced fx if the pt will not tolerate prolonged cast immobilization (e.g. professional athletes and manual laborers )
ORIF of scaphoid fractures can be done by many ways : - K-wires ( easy insertion ) - Herbert screws - AO screws - Staples AO SCREW Herbert screw
Treatment of middle third fxs - commonest (65%) - If stable: short-arm thumb spica cast - If undisplaced fx older than 3 wks : long-arm thumb spica cast - If displaced : ORIF (k-wires or screws)
Proximal Pole Fractures • If it is a fresh fx, can be fixed by 2-3 k-wires • Alternatively ,one may use a Herbert screw
Distal Pole Fractures • undisplaced should heal in 4-8 wks in a cast • Displaced fx needs ORIF
Complications of Scaphoid Fx • Delayed union or Nonunion • Malunion (Humpback deformity) • SLAC wrist • Osteonecrosis Treatment of Nonunion • Bone grafting
Malunion • occur when a displaced or angulated fracture is allowed to heal without anatomic reduction • In most of cases , there is a dorsal angulation resulting in a fixed humpback deformity • Treatment : -osteotomy, bone graft,and internal fixation
SLAC • scapholunate advanced collapse (SLAC) refers to a specific pattern of osteoarthritis and subluxation which results from untreated chronic scapholunate dissociation or from chronic scaphoid nonunion