Download
1 / 34
340 likes | 494 Views
Laparoscopic Gastric Bypass should be the Gold Standard. Diclosure Slide. Honorarium for talks and Mentoring from Covidien and J&J Honorarium for talk Nestles. Laparoscopic Gastric Bypass should be the Gold Standard. Dr. John Hagen Assistant Professor of Surgery University of Toronto.

E N D
Diclosure Slide • Honorarium for talks and Mentoring from Covidien and J&J • Honorarium for talk Nestles
Laparoscopic Gastric Bypass should be the Gold Standard Dr. John Hagen Assistant Professor of Surgery University of Toronto
Humber River Regional Hospital • 500 bariatric operations per year • Over 90% are gastric bypasses • 10% are gastric sleeve resections • < 1% are bands
U of T affiliation • Part of the U of T general surgery residency and MIS fellowship programs • Usually have 2 fellows and 2 residents • Every case is done with a trainee
Laparoscopic Gastric Bypass is the Gold Standard • Gastric Banding, Sleeve Resections, Vertical banded gastroplasty- Restrictive • Duodenal switch- Malabsorbtive
Restrictive operations • Idea is that the stomach will only allow a small quantity to enter • Classic operation in the 1980’s • Vertical Banded Gastroplasty
Historical failure of VBG • 56% of patients will require revisional surgery after VBG over 12 years • 12% of open RYGB require revisional surgery • Failed VBGs are best treated by RYGB Failed VBG are best treated by RYGBObes Surg. 1998 Feb;8(1):21-8. Revisional surgery after failed vertical banded gastroplasty: restoration of vertical banded gastroplasty or conversion to gastric bypass. van Gemert WG, van Wersch MM, Greve JW, Soeters PB.
Similar? Adjustable gastric band Vertical gastroplasty
Given enough time banding will fail • Over a 12 year period 1 out of 3 patients experienced band erosion • 50% required removal of the band • Re-operation rate of 60% Long-term outcomes of laparoscopic adjustable gastric banding. Himpens J, Cadière GB, Bazi M, Vouche M, Cadière B, Dapri G. Arch Surg. 2011 Jul;146(7):802-7.
Canadian experience • LRYGBP compared to LAGBD • Dr. N. Christou from McGill University • 1035 procedures performed • “Superior weight loss and low revision requirement for the LRYGBP making this a more durable operation in a publically funded health care system” Five-year outcomes of laparoscopic adjustable gastric banding and laparoscopic Roux-en-Y gastric bypass in a comprehensive bariatric surgery program in Canada.Christou N, Efthimiou E. Can J Surg. 2009 Dec;52(6):E249-58
Duodenal Switch • Malabsoptive • Requires close follow up • Patients may have 20 foul smelling bowel movements per day • Tight balance between weight loss and malnutrition and micronutrient deficiency • Technically difficult • In the US, 2% of all bariatric operations
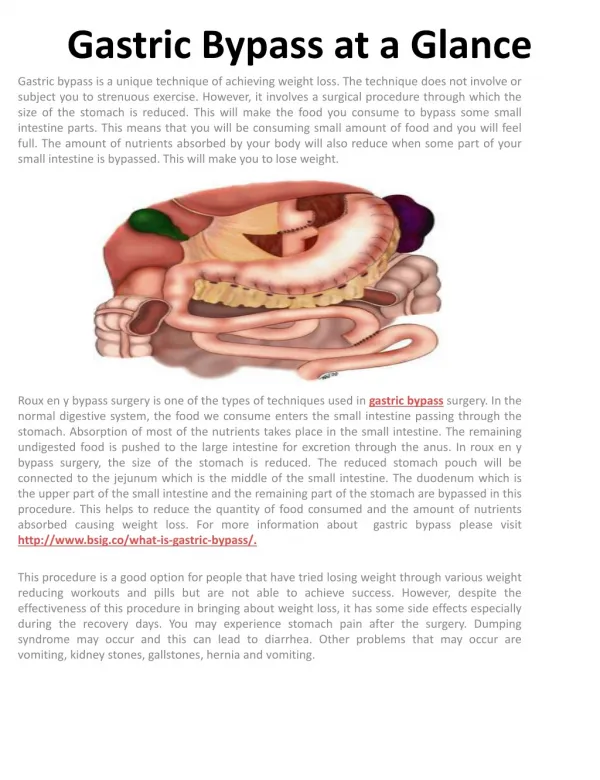
Gastric Bypass 1967- University of Iowa -Gastric Bypass surgery developed after observing massive weight loss following gastrectomy
Evidence based opinion Ann Surg. 2011 Sep;254(3):410-20; discussion 420-2. First report from the American College of Surgeons Bariatric Surgery Center Network: laparoscopic sleeve gastrectomy has morbidity and effectiveness positioned between the band and the bypass. Hutter MM, Schirmer BD, Jones DB, Ko CY, Cohen ME, Merkow RP, Nguyen NT.
Objective of paper • To assess the safety and effectiveness • Sleeve (LSG) • Adjustable Gastric Band (LAGB) • Laparoscopic Gastric Bypass(LRYGB) • Open Gastric Bypass (ORYGB)
Data collection-28,616 patients • ACS Bariatric Surgery Center Network • Prospective, longitudinal data system • Univariate and Multivariate analysis • 30 day, 6 month, and 1 year outcomes • Morbidity and mortality, readmission rates, reoperations, reduction in BMI and comorbidities
Data collected from 7/2007 to 9/2009 • 109 centers • 28,616 patients
Conclusions • LSG has a higher risk-adjusted morbidity, readmission and reoperative rates compared to LAGB, but lower re-operation/intervention rates compared to LRYGPB
Reduction in BMI and co-morbidities • Best- LRYGBP • 2nd best- LSG • 3rd best- LAGB
Long term results • Gastric bypass has the most information on long term results • Operation has been performed as the gold standard for 20 years • Excellent data from Canadian experience
Impact on Mortality? • Christou, et al, Annals of Surgery, Sept 2004 (Quebec) • Five year observational 2-cohort study comparing patients treated with bariatric surgery without comorbidities at the time of surgery • Surgical group (n=1035) • Open gastric bypass (79.2%) • Open vertical banded gastroplasty (18.7) • Laparoscopic gastric bypass (2.2%) • Mean age: 45.1 • Mean initial BMI: 50.0 • EWL: 67% • Control group (n=5746) • Mean age: 46.7 • Initial BMI > 40
Recent NEJM Article #2 • Sjostrom et al., Aug 2007 • Prospective • 2010 patients had surgery • 2037 conventional (non-surgical) treatment • Average 10.9 year follow-up
NEJM, Aug 2007 (#2) Total weight loss: 1 – Bypass, 2 – VBG, 3 - Adj Band
LRYGBP is the Gold Standard • Best reduction in BMI and co-morbidities • Low mortality rates • Easy to perform once trained