Download
1 / 66
690 likes | 915 Views
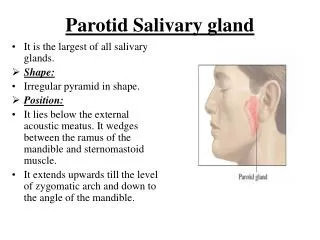
Salivary gland tumours. Investigations and Management. CHRISTY CATHREEN THOMAS. INVESTIGATIONS. FNAC SIALOGRAPHY C T SCAN CT SCANNING WITH SIALOGRAPHY MRI TECHNICIUM SCANNING ANGIOGRAPHY BIOPSY. FNAC. ACCURACY- 84-97%. SENSITIVITY- 95% SPECIFICITY- 86-100%

E N D
Salivary gland tumours Investigations and Management CHRISTY CATHREEN THOMAS
INVESTIGATIONS • FNAC • SIALOGRAPHY • C T SCAN • CT SCANNING WITH SIALOGRAPHY • MRI • TECHNICIUM SCANNING • ANGIOGRAPHY • BIOPSY
FNAC ACCURACY- 84-97% SENSITIVITY- 95% SPECIFICITY- 86-100% Safe&well tolerated EFFICACY –well established
Safe alternative to open biopsy. <18 G needle is used – no risk of seeding. RARELY ALTERS THE SURGICAL MANAGEMENT &may only influence treatment planning.
fnac • . To differentiate b|w neoplastic & nonneoplastic processes. • Important to distinguish benign&malignant neoplasm • Useful for preoperative patient counselling. • For surgical planning. • To avoid surgery in large no. of patients.
C T SCAN • EXTENT OFINVOLVEMENT. left parotid
Sialography • Little value in tumour assessment. • DEEP LOBE INVOLVEMENT. • whether or not a mass is within the duct.
Sialography • Sialography must be performed by an EXPERIENCED RADIOLOGIST since artefacts can be created by TRAUMATIC CANNULATION & OVERFILLING THE GLAND WITH CONTRAST MATERIAL.
CT SCANNING WITH SIALOGRAPHY • SHOWS DEEP LOBE DISPLACEMENT. • REVEALS FILLING DEFECTS IN THE SUPERFICIAL LOBE.
MRI SCANNING • EXTENT OF deep lobe INVOLVEMENT. • any other associated SOFT TISSUE ABNORMALITIES
MRI I
TECHNICIUM SCAN • Abramson et al in 1969 used --To differentiate “ hot” Warthin’s tumour from “cold”mixed tumours & other neoplasms. • Helps to identify Deep lobe in doubtful cases.
ANGIOGRAPHY • in tumours of PARAPHARYNGEAL SPACE – help to differentiate SALIVARY GLAND tumours from – paragangliomas of the carotid bodies Or Nerve sheath tumours . Both of which have a characteristicTUMOUR CIRCULATION • It also allows IDENTIFICATION OF FEEDING VESSELS
BIOPSY • Incisional biopsy should NOT be done in case of a DISCRETE SALIVARY GLAND MASS - since most of the solitary parotid masses are PLEOMORPHIC ADENOMAS ,incising it is UNNECESSARY for diagnosis & it will almost certainly lead to later RECURRENCE
Biopsy • The only acceptable biopsy in such cases is PAROTIDECTOMY • Incisional biopsy is warranted –when there is SKIN INVOLVEMENT & probable MALIGNANCY,also for large lesions in oral cavity
Biopsy-Risks • Bleeding • Infection • Injury to facial and trigeminal nerve • Allergic reaction to anaesthetic
MINOR SALIVARY GLAND TUMOURS • Surface tumours---so INCISIONAL BIOPSY is to be prefered to excisional biopsy This policy carries NO RISK OF IMPLANTATION; but patients with benign tumours will be subjected to a LATER LOCAL EXCISION.
History Salivary gland surgery dates back to the 16th century. The anatomy of the parotid gland and the role of the main ducts were described in the mid-17th century. The earliest references to "para-auricular swellings," as the Greeks Between 1650 and 1750, salivary gland surgery was limited to the treatment of ranulas and oral calculi.
Parotids - malignant • Treatment is based on • grade of the tumor. • metastases. • histologic type. • Total parotidectomy with preservation of the nerve.
Parotids - malignant • Involvement of a branch of the nerve – removal of that branch. • Young patients - nerve graft to replace resected nerve segment to avoid long-term sequelae of facial nerve palsy
Benign tumors • Benign tumors of the superficial lobe -removed with a clear margin by superficial lobectomy.
If the deep lobe is involved, total parotidectomy. Partial parotidectomy is sometimes possible.
Node positives • Neck dissection Radical neck dissection if there is involvement in the sternocleidomastoid muscle or the jugular vein. Modified or selective neck dissection depending on the site of metastasis.
Therapeutic removal of the regional lymphatics is indicated when clinical adenopathy is present
Submandibular • Same basic rules as for parotids. • Managed by en-bloc resection of the gland plus the submental and submandibular lymph nodes. • Preservation of marginal mandibular, hypoglossal, and lingual nerves, for benign tumors.
Radical resection of the nerves, underlying muscle, platysma, skin, and for extensive local invasion. Adjuvant postoperative radiotherapy.
Minor salivary glands • Therapy is wide local resection, including subjacent bone if involved, with adjuvant radiotherapy for malignancy.
Cervical lymphadenectomy for patients with histologically proved lymph node metastases. Palatal defects -dental prostheses extensive disease -local or distant tissue transfer.
Pleomorphicadenoma Complete surgical excision with a surrounding margin of normal tissue. • ENUCLEATION • high local recurrence • Rupture of the capsule and tumour spillage in the wound increase the risk of recurrence.
Warthin’s tumour • Superficial parotidectomy with facial nerve preservation. • spillage in the wound increase the risk of recurrence.
Oncocytoma • Surgical excision with a margin of normal tissue. • Low rate of recurrence if removal is complete. • Enucleation or curettage is not appropriate.
Monomorphic adenoma • nonaggressive behavior. • Surgical excision isadequate Myoepitheliomas • benign behavior. • Complete surgical excision is appropriate
Mucoepidermoid carcinoma • Stage I and II • surgical excision alone. • Stage III and IV • radical excision. • a neck dissection. • postoperative radiation therapy.
Adenoid cystic carcinoma • Complete surgical resection and postoperative radiation. • recurrence rates - 42%. • Chance for distant metastasis, common site being the lung. • Prognosis for complete cure is poor.
Acinic cell carcinoma • Surgical excision. • Postoperative radiation. • Minor salivary glands, a portion of the maxilla or mandible may have to be resected with the tumor. • Neck dissection in node positives.
Carcinosarcoma Carcinosarcoma • Radical surgery. • Neck dissection for palpable nodes and postoperative radiation.
Squamous cell carcinoma Aggressive with rapid growth, rapid spread to lymph nodes. Surgical resection, neck dissection and post operative radiation. Surgical resection, neck dissection and post operative radiation. Surgical resection, neck dissection and post operative radiation.
Squamous cell carcinoma • Surgical resection. • neck dissection. • post operative radiation.
Undifferentiated Carcinoma • complete surgical excision with neck dissection for palpable nodes. • Postoperative radiation therapy. • Chemotherapy
Superficial Parotidectomy Indications:- Benign tumours or low-grade malignant tumours of small size. without involvement of the facial nerve in the superficial lobe of the parotid gland. c/c inflammation of parotid gland, resistant to conservative treatment. Tumour-like lesions in the parotid. nodular Sjögrens syndrome. oxyphilic lymphogranuloma.
General anasthesia or • Local anaesthesia with 1% Lidocain containing adrenaline.
Incision Modified Blair incision "lazy“ S incision
Deepening of incision to parotid fascia dividing platysma. • Plane of cleavage between external auditory meatus and gland opened up with blunt-pointed curved scissors. • Parotid fascia dissected till sternomastoid.
The posterior branch of the great auricular nerve should be preserved unless the tumour involves the nerve or the nerve adheres to the tumour.
Three approaches are used :- • Anterograde approach • By tracing the main trunk of the favial nerve and dissecting out the gland towards the terminal branches. • Retrograde • By tracing the terminal branches and dissecting out in the opposite direction. • By guiding through the direction of the facial vein.
How to identify facial nerve?. Tragal pointer:- 1-1.5 cm deep and inferior. Tympanomastoid suture:- 6-8cm medially. Posterior belly of digastric:- superior to insertion. Styloid process:- postero-lateral to base. Retrograde tracing. Cortical mastoidectomy.
Stensen’s Duct is used as a landmark for the identification of the buccal branches of the facial nerve. Relationship among (1) the buccal branch of the facial nerve, (3) parotid duct (2) the accessory gland