Download

1 / 53
600 likes | 1.54k Views
DISEASES OF SALIVARY GLAND. Introduction. Two types of salivary glands - Major glands and minor glands Major: parotid, submandibular & sublingual Minor: lingual, palatal, labial, buccal etc Type of cells: Serous , mucous & myoepithelial cells Heterogenous group of lesions

E N D
Introduction • Two types of salivary glands - Major glands and minor glands • Major: parotid, submandibular & sublingual • Minor: lingual, palatal, labial, buccal etc • Type of cells: Serous , mucous & myoepithelial cells • Heterogenous group of lesions • Morphologic variation • Common lesions
HISTOLOGICAL CLASSIFICATION OF SALIVARY GLAND TUMOURS ADENOMAS PLEOMORPHIC ADENOMA MYOEPITHELIOMA BASAL CELL ADENOMA WARTHIN TUMOUR ONCOCYTOMA CANACLICULAR ADENOMA SEBACEOUS ADENOMA DUCTAL PAPILLOMA .INVERTED DUCTAL PAPILLOMA .INTRADUCTAL PAPILLOMA .SIALADENOMA PAPILLIFERUM CYSTADENOMA .PAPILLARY CYSTADENOMA .MUCINOUS CYSTADENOMA
CARCINOMAS • 1-ACINIC CELL CARCINOMA2-MUCOEPIDERMOID CARCINOMA3-ADENOID CYSTIC CARCINOMA4-POLYMORPHOUS LOW GRADE ADENOCARCINOMA5-EPITHELIAL-MYOEPITHELIALCARCINOMA6-BASAL CELL ADENOCARCINOMA7-SEBACEOUS CARCINOMA8-PAPILLARY CYSTADENOCARCINOMA9-MUCINOUS ADENOCARCINOMA10-MALIGNANT MYOEPITHELIOMA11-CARCINOMA IN PLEOMORPHIC ADENOMA12-SQAMOUS CELL CARCINOMA13-SMALL CELL CARCINOMA14-UNDIFFERENTIATED CARCINOMA
NON EPITHELIAL TUMOURMALIGNANT LYMPHOMASSECONDARY TUMOURSUNCLASSIFIED TUMOURS TUMOURLIKE LEISIONSIALADENOSIS ONCOCYTOSISNECROTIZING SIALOMETAPLASIA BENIGN LYMPHOEPITHELIAL LEISION Mikulcz’s syndrome & Sjogren’s syndrome SALIVARY GLAND CYSTS CHRONIC SCLEROSING SIALADENITIS OF SUBMANDIBULAR GLAND CYSTIC LYMPHOID HYPERPLASIA IN AIDS
PLEOMORPHIC ADENOMA • Most common salivary gland tumor • Pleomorphism – more than one form • It is also called as mixed tumor but is not a true mixed tumour, • Consist of cells exhibiting the ability to differentiate to epithelial (ductal & nonductal) & mesenchymal (chondroid,myxoid & osseous). • Myoepithelial & reserve cell in the intercalated duct are responsible for • histogenesis. • PLAG1 gene
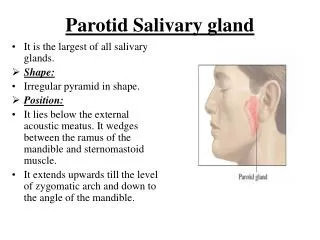
Pleomorphic adenoma Clinical features • Appears as painless, slowly growing, firm mass, sometimes showing intermittent growth, no fixation. • Majority of lesion found in 4th & 6th decade of life • Parotid gland is the most common site (90% ) • Palate is most common intra oral site
Histopathology • Macroscopic features • Irregular to ovoid mass with well defined borders. • In major gland- either incomplete fibrous capsules or uncapsulated. • In minor gland – uncapsulsted. • Cut surface is rubbery, fleshy, mucoid or glistening with homogenous tan or white color .
Microscopic features • Morphologic diversity is the most characteristic features • Categories of tumors • 1-Principally myxoid • 2-Myxoid & cellular component present in equal proportion. • 3-Predominantly cellular. • 4-Extremely cellular. • Epithelium often forms ducts & cystic structures or may occurs as islands or sheets of cells. • Some Myoepithelialcells resemble plasma cells(also called as hyaline cells) • Extensive accumulation of mucoid material around myoeoithelial cells gives a myxoid appearance. • Vacoulardegenaration of cells in these areas can produce a chondroid and osseous appearance. • When tumor is composed entirely of myoepithelial cells with no ductalelements.such tumor are often called as myoepitheliomas.
BASAL CELL ADENOMA • Because of its uniform histopathologic appearance, it is classified as monomorphic adenoma. • It is neoplasm of a uniform population of basaloid epithelial cells arranged in solid, trabecular, tubular, or membranous patterns. • It shows some histologic similarity to the canalicular adenoma.
Microscopic features On the basis of morphologic appearance it divided into 4 subtypes 1. Solid 2.Tubular 3.Trabecular 4.Membraneous
Canalicular adenoma • Less common tumor occurs almost exclusively in the minor salivarygland. • It composed of columnar epithelial cells arranged in single or double layer forming branching cords in a loose stroma. • Striking predilection for the upper lip,
Clinical features • Striking predilection for the upper lip, buccal mucosa is the second most common site. • More common in females with the ratio of 1.8:1. • It generally presents as a slowly growing ,well-circumscribed ,firm nodule. • Overlying mucosa may be normal in color or bluish & can be mistaken for a mucocele.
Histologic features • It is composed of long columns or cords of cuboidal or columnar cells in a single layer. • Sometimes rows of cells are closely approximated & appears as a double row of cells showing a ‘party wall’ appearance. • Supporting stroma is loose and fibrillar with dilate vasclurity.
Warthin’s tumor (Papillary cystadenoma lymphomatosum) • Second most common tumor . • Occur almost exclusively in parotid gland occasionally in submaxillary gland. • Smokers have an eightfold greater risk . • Epstein-Barr virus is also implicated in pathogenesis.
Clinical features • Appears as a slowly growing, painless, nodular mass of the parotid. • Commonly present in the sixth & seventh decades.in 5% to 14% of cases occurs bilaterally • It is consider as a disease of male, male- to- female ratio is 10:1.
Histologic features Macroscopic features • Smooth, soft & well encapsulated when located in parotid. • Tumor contain variable no. of cysts that contain a clear fluid. • Microscopic features • Tumor is composed of mixture of ductal epithelium & lymphoid stroma. • It is adenoma exhibiting cyst formation, with pappilary projections into the cystic spaces & a lymphiod matrix showing germination centers. • Cyst are lined by papillary proliferation of bilayered oncocytic epithelium. • Focal areas of sqamous metaplasia & mucous cell prosoplasia may be seen.
Acinic cell carcinoma • It is a malignant epithelium neoplasm in which the neoplastic cells express acinar differentiation. • It has a low-grade malignant potential.
Clinical features • It closely resemble the pleomorphic adenoma in gross appearance, tending to be encapsulated & lobulated. • More than 80% of cases occurring in parotid. • Most common intraoral sites are lips & buccal mucosa. • Women are affected more commonly than men ( 3:2 ). • Tumor present as a slowly growing, mobile or fixed mass of various durations. • Facial muscle weakness may be seen.
Histologic features • It is frequently surrounded by a thin capsule, may be composed of cells of varying degree of differentiation. • Most characteristic cell has features of the serous acinar cells, with abundant basophilic cytoplasm & a round darkly stained eccentric nucleus. • Growth patterns • 1. Solid • 2. Micro-cystic • 3. Papillary cystic • 4. Follicular
Solid : consist of numerous well-defferentiated acinar cells arranged in a pattern that resembles normal parotid tissue. • Micro-cystic : multiple small cystic spaces are created that may contain mucinous or eiosinophlic material. • Papillary cystic: larger cystic areas are formed that are lined by epithelium having papillary projection into cystic spaces. • Follicular: It has appearance similar to that of a thyroid tissue .
Mucoepidermoid carcinoma • Tumor is composed of both mucous secreting & epidermoid type cells in varying proportions. • Most common malignant neoplasm in major & minor salivary gland (29 % to 30 % of malignant tumor ). • Most common salivary gland tumor seen in children • Parotid is most common site of occurrence.
Clinical features • It occurs with slight female predilection. • Occurs primarily in the third or fifth decade of life. • Prior exposure to the ionizing radiation increase the risk of this tumor. • It is not encapsulated, but tends to infiltrate the surrounding tissue, it metastasize to the regional lymph nodes. • Distant metastases to lung, bone, brain, subcutaneous tissue are also common.
Histologic features • Mucous cells vary in shape but contain abundant foamy cytoplasm that stains positive with mucin stains. • Epidermoid cells have sqamoid features, demonstrate a polygonal shape, intercellular bridges & rarely keratinization. • In addition, a third type of cells is typically present – the intermediate cell. This cell is basaloid in appearance & is believed to be a proginator of the mucous & epidermoid cells. Tumor is divided into 3 histopathologic grade on the basis of following Amount of cystic formation. Degree of cytologic atypia. Relative no. of mucous, epidermoid, intermediate cells.
Low- grade : Show well formed glandular structure & prominent mucin filled cystic spaces, minimal cellular atypia, & a high proportion of mucous cells. Intermediate- grade : Tumor have solid areas of epidermoid cells or sqamous cells with intermediate basaloid cells. - cyst formation is seen but less prominent than low grade tumor. - all type of cells are present but intermediate cells predominate. High- grade : Consist of solid island of squamous & intermediate cells, which can demonstrate considerable pleomorphism & mitotic activity. - cystic component is usually very less. - necrosis & perineural invasion may be present.
Adenoid cystic carcinoma (cylinderoma) • Fifth most common malignant tumor • It is a slow- growing but aggressive neoplasm with remarkable capacity for recurrence. • It has a marked tendency to spread through perineural spaces.
Histologic features It is composed of myoepithelial cells & ductal cells which have a varied arrangement. Growth pattern Cribriform pattern :shows basaloid epithelial cells nests that form multiple cylindrical cyst like pattern resembling swiss cheese or honey comb pattern. Tubular pattern : Reveals tubular structures that are lined by stratified cuboidal epithelium. Solid pattern :Shows solid groups of cuboidal cells with little tendency towards duct or cyst formation.
Cribriform pattern is most common, where as solid pattern is the least common. Solid pattern has up to 100% recurrence rate as compared with 50-80% for the tubular & cribriform variant.
Carcinoma in plemorphic adenoma(Malignant mixed tumors) • This uncommon neoplasm is divided into three categories • Carcinoma ex pleomorphic adenoma • Carcinosarcoma • Metastasizing mixed tumor 1-Carcinoma ex pleomorphic adenoma • It occurs when a carcinoma develops from the epithelial component of a pre xistingpleomorphic adenoma. • It is 6th most common malignant salivary gland tumor.
2-Cacinosarcoma (true malignant mixed tumor) • Rare malignant salivary neoplasm. • It contain both the stromal & epithelial elements. 3-Metastasizing mixed tumor • It refers to an otherwise benign acting plemorphic adenoma that develops metastatic deposits.
Sjogren's syndrome (sicca syndrome) • This is a common condition affecting the salivary glands. • Two types: • Primary (sicca complex)- dry eyes & dry mouth. • Secondary - dry eyes dry mouth along with systemic lupus erythematosus, polyarteritisnodosa, polymyositis or scleroderma. • Consists of a triad of • Keratoconjunctivitissicca • Xerostomia • Rheumatoid arthritis
Etiology- genetic, hormonal, infectious (EB virus, cytomegalo virus), immunlogical, autoimmune. • Clinical features • Common in female (F:M=10:1) • Dryness of mouth & eyes • Pain and burning sensation of oral mucosa • Difficulty in swalloing • Altered taste & difficulty in wearing denture • Tongue becomes fissured and exhibit atrophy of papilla
Histological features • 3 types of alterations are present • Intense lymphocytic infiltration of the gland replacing all acinar structures although the lobular architecture is preserved. • Proliferation of ductal epithelium & myoepithelium to form “epimyoepithelial islands” • Simple atrophy of gland sequential to the lymphocytic infiltration. • Radiographic features- • sialographs demonstrate the formation of punctate, cavitary defects which are filled with radiopaque contrast media. These filling defects produce “cherry blossom” or “branchless fruit -laden tree”.
Lab investigations • Schirmer’s test – less than 8 mm wetting per 5 mins • Rose bengal staining - cornea or conjuctiva to demonstrate keratoconjunctivitis sicca • Elevated rheumatoid factor - > 1: 320 • Elevated anti nuclear antibody (ANA) – > 1:320 • Presence of anti SS-A(Ro) & anti SS-B (La) antibodies
Benign lymphoepithelial lesion (Mikulicz syndrome) • Similar to sjogrens syndrome • Considered by many to be a type of sjogrens syndrome • It is characterized by the abnormal enlargement the salivary & lacrimal gland. • the patient are at hightened risk for developing lymphomas. Etiology • Exact cause is unknown but suspected to be an autoimmune disorder.
Clinical features • It affects more females than males. • Often occurs in combination with Sjogren syndrome. • It is characterised by sudden onset of xerostomia, other syptoms includes inlarged lacrimal gland, painless swelling of salivary gland(parotid & submaxillary). • Some people may experience recurring fever. • Histologic features • It shows a heavy lymphocytic infiltrate associated with the distruction of the salivary acini. • The ductal cells and surrondingmyoepithelial cells become hyperplastiv, forming highly characteristic groups of cells known as ‘epimyoepithelial islands.
Nectrotizingsialometaplasia (salivary gland infarction) • It is nonneoplastic inflammatory condition of the salivary gland. Etiology • It is the result of ischemia of the salivary tissue that leads to local infarction. • Predisposing factor • Traumatic injuries • Dental injections • Ill- fitting dentures Clinical features • It most frequently develops in the palatal glands. • Male : female=2:1 • Typical presentation is crateriform ulcer of the palate
Histologic features • Charaterized by acinar necrosis in early lesion, followed by associated squamous metaplasia of salivary ducts. • There may be a liberation of mucin, with an associated inflammotary response. • Squamous metaplasia of epidermoid cells along with mucous cells mimics mucoepidermoid carcinoma • Squamous cells within the connective tissue also mimics the histologic appearance of squamous cell carcinoma.
SIALOLITHIASIS Sialolithiasis is the occurrence of calcific deposits (stones) in salivary gland or its ducts. CLINICAL FEATURES: • Patients complain of moderately severe pain, particularly just before and during meals, owing to psychic stimulation of salivary flow associated with swelling of salivary gland. • Occlusion of duct prevents free flow of saliva and this stagnation under pressure produces pain and swelling. • They may be demonstrated by roentgenogram. • It may occur at any age, most common in middle aged adults.
Most commonly occur in submandibular gland duct because of its • tortuous course of duct • upward course. • More mucous secretion TREATMENT AND PROGNOSIS: • Small calculi can be removed by manipulation. • If they are present near or in substance of gland , then surgical extirpation of the gland may be necessary, • Solitary sialolith does not usually recur
Mucocele Common lesion of oral mucous membrane Two types Mucous extravasation cyst Mucous retention cyst Mucous extravasation cyst: caused due to trauma to the duct leading to its rupture and spilling of saliva into the connective tissue stroma. Not a true cyst , as it lacks epithelial lining. Depending on location it can be Superficial Deep
Mucous retention cyst: Caused by blockage of the salivary gland duct – leading to pooling of saliva within the duct. • as the saliva gradually increases the duct also enlarges resulting in a true cyst which is lined by ductal epithelium. • Treatment : surgical excision along with the minor salivary gland.
RANULA • Derived from the word –RANA (frog’s belly) • It is a form of mucocele , which occurs in floor of mouth. • Types • Superficial • Deep (plunging)