Download
1 / 36
440 likes | 1.93k Views
Chapter 22 – Mycobacterium tuberculosis & Other Nontuberculous Mycobacteria. MLAB 2434 – Clinical Microbiology Cecile Sanders & Keri Brophy-Martinez. General Characteristics. Slender, slightly curved or straight rod-shaped organisms Non-motile Do not form spores

E N D
Chapter 22 – Mycobacterium tuberculosis & Other Nontuberculous Mycobacteria MLAB 2434 – Clinical Microbiology Cecile Sanders & Keri Brophy-Martinez
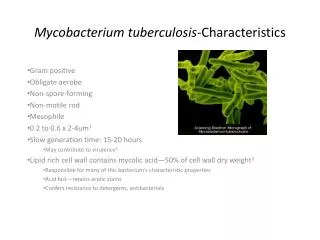
General Characteristics • Slender, slightly curved or straight rod-shaped organisms • Non-motile • Do not form spores • Cell wall with extremely high lipid content • Staining requires longer time or application of heat • Once stained, resist decolorization with acid-alcohol (acid-fast)
General Characteristics (cont’d) • Strictly aerobic • Grow more slowly than most bacteria • Traditional characteristics used to identify Mycobacterium • Rate of growth • Colony morphology • Pigment production • Nutritional requirements • Optimum incubation temperature • Biochemical test results
General Characteristics (cont’d) • Newer techniques • Automated culture system, such as BACTEC • Nucleic acid probes with PCR • Thin-layer chromatography • GLC • High-performance liquid chromatography
Safety Considerations • Mycobacteriology workers are three times more likely to seroconvert (develop positive skin test) • Adequate safety equipment • Safe laboratory procedures training • Information on hazards • Preparations for unexpected accidents • Staff must be monitored regularly by medical personnel
Safety Considerations (cont’d) • Skin test • Also called “Mantoux test” and PPD • Those with positive skin test must be advised to have chest X-ray • Proper Ventilation • Separate from other parts of lab • Negative air pressure (6 to 12 room air changes/hour)
Safety Considerations (cont’d) • Biological Safety Cabinet • Use of Proper Disinfectant • Bactericidal for mycobacteria • Also called “tuberculocidal” • Other precautions • Disposables • Protective clothing, face masks
Specimen Collection and Processing • Variety of clinical specimens, including respiratory, urine, feces, blood, CSF, tissues, and aspirations • Should be collected before antibiotic therapy and processed ASAP • Sputum is most common; should be collected in a wide-mouth container to avoid aerosols
Specimen Collection and Processing (cont’d) • Sputum • Number of specimens needed is inversely related to the frequency of smear positivity • Should be from a deep cough or expectorated sputum induced by neubulization • Bronchial washings or lavages may be collected
Specimen Collection and Processing (cont’d) • Gastric aspirates • Used to recover mycobacterium that may have been swallowed during the night • Only used when patient is unable to produce a good quality sputum specimen • Urine – First morning preferred
Specimen Collection and Processing (cont’d) • Stools – primarily collected from AIDS patients to determine Mycobacterium avium complex (MAC) • Blood – most commonly from AIDS and other immunosuppressed patients • Tissues and other body fluids – need a fairly large volume of CSF, since number of organisms in that site are rare
Digestion & Decontamination of Specimens • Because Mycobacterium grow so slowly and are often collected from non-sterile body sites, they are easily overgrown by other bacteria • Specimens from non-sterile sites, therefore, must be “decontaminated” • Sputums or other viscous specimens also must be “digested” • Specimens from sterile sites (CSF, etc.) do not need decontamination
Digestion & Decontamination of Specimens (cont’d) • Decontamination • Specimen from non-sterile site is mixed with an agent that will kill non-mycobacterium bacteria • Common decontamination agents • NaOH is most common • Benzalkonium chloride (Zephiran) • Oxalic acid • After decontamination, the agent must be neutralized so that it will not eventually kill the Mycobacterium
Digestion & Decontamination of Specimens • Digestion • Liquefying mucus enables the mycobacterium to contact and use the nutrients in the agar medium • Common digestion agents • N-acetyl-L-cysteine – most common • Trisodium phosphate (Z-TSP) – used with Zephiran
Concentration • After decontamination and digestion, the specimen is centrifuged in a closed, vented centrifuge to concentrate the organisms
Acid Fast Stains • After centrifugation, the button at the bottom of the tube is used to make a smear and to inoculate media • Acid Fast Stains • Ziehl-Neelsen – uses heat to drive the color into the lipids of the cell wall; decolorized with acid-alcohol • Kinyoun – cold stain • Auramine or auramine-rhodamine fluorochrome stain – more sensitive • After staining, a minimum of 300 oif are examined
Culture Media and Isolation Methods • Mycobacterium are strictly aerobic • Slow growers; cultures held for 6 weeks before calling negative • Media • Lowenstein-Jensen (LJ) media – egg based • Middlebrook 7H10 and 7H11 agar – serum based • Middlebrook 7H9 broth
Culture Media and Isolation Methods (cont’d) • Labs with large volumes of Mycobacterium cultures use an automated reader (BACTEC) • BACTEC broth contains 14C-labeled substrate • When organisms grow, 14C in the form of 14CO2 is released and detected radiometrically
Laboratory Levels or Extents of Service for Mycobacterium • American Thoracic Society levels • 1. Specimen collection only • 2. Acid-fast stains and/or inoculation only • 3. Isolation and presumptive identification of Mycobacterium species • 4. Definitive identification and antibiotic sensitivity testing
Identification of Mycobacterium • Colony Morphology • Either smooth and soft or rough and friable • Growth rate • Rapid growers – colonies in < 7 days • Slow growers – colonies in > 7 days • Temperature
Identification of Mycobacterium (cont’d) • Photoreactivity • Photochromogens – produce carotene pigment upon exposure to light • Scotochromogens – produce pigment in light or dark • Nonchromogenic – no pigment; these colonies are a buff color
Identification of Mycobacterium (cont’d) • Biochemical Identification • Most labs now use nucleic acid probes with or without PCR • Older tests • Niacin accumulation • Nitrate reduction • Catalase • Hydrolysis of Tween 80 • Iron uptake • Arylsulfatase
Identification of Mycobacterium (cont’d) • Older tests (cont’d) • Pyrainamidase • Urease • Inhibitory tests • NAP • TCH • Growth in 6.5% NaCl • Tellurite reduction • Growth on MacConkey
Antibiotic Sensitivity Testing for Mycobacterium • These tests must be performed with great attention to detail, because Mycobacterium is fairly resistant and only a few organisms left can cause reinfection • Development of drug-resistance • Common antibiotics (usually two or more are given) • Isoniazid • Rifampin • Ethambutol • Streptomycin • Pyrazinamide
Mycobacterium Infections • Truly pathogenic • M. tuberculosis • M. bovis • M. ulcerans • Potential pathogens • M. kansasii • M. marinum • Other possible pathogens and rare pathogens listed on p. 670
Mycobacterium tuberculosis • Primarily a pathogen of the respiratory tract (“TB”) • One of the oldest communicable diseases • Over 1 billion cases worldwide, with 8 to 10 new cases each year and 3 million deaths per year • Once called “consumption”
Mycobacterium tuberculosis (cont’d) • Primary tuberculosis • Spread by coughing, sneezing, or talking • Inhaled into alveoli, where the organisms are phagocytized • If the organism does not cause immediate infection, the organism can be “walled off” in a granuloma • Granulomas can break down in future and the organisms can cause infection later
Mycobacterium tuberculosis (cont’d) • PPD Test
Mycobacterium tuberculosis (cont’d) • PPD Test (cont’d) Positive Test
Mycobacterium tuberculosis (cont’d) • Extrapulmonary tuberculosis • Spleen • Liver • Lungs • Bone marrow • Kidney • Adrenal gland • Eyes
Mycobacterium tuberculosis (cont’d) • Identification • Slow grower • Colonies are thin, flat, spreading and friable with a rough appearance • May exhibit characteristic “cord” formation • Grows best at 35 to 37° C • Colonies are NOT photoreactive
Other Mycobacteria • Mycobacterium bovis – primarily in cattle, dogs, cats, swine, parrots and human; disease in humans closely resembles M. tuberculosis • MOTT (Mycobacteria Other Than Tubercle Bacillus) or NTM (Nontuberculous mycobacteria) • Most found in soil and water • Chronic pulmonary disease resembling TB
Other Mycobacteria (cont’d) • NTM (cont’d) • M. avium Complex (MAC) • M. kansasii • Mycobacterium fortiutum-chelonei Complex • M. marinum • Etc., etc.
Mycobacterium leprae • Causes leprosy or Hansen’s Disease • Infection of the skin, mucous membranes and peripheral nerves • Most cases are from warm climates • Bacteria infect the cooler areas of the body (ears, nose, eyebrows, fingers, toes) • Diagnosis made from finding acid-fast bacilli in scrapings from lesions • Not culturable, except in mouse foot pads