Download

1 / 59
610 likes | 903 Views
Respiratory Tract Infections Common cold Acute and chronic bronchitis Pneumonia (CAP and VAP). דר רות אורני-וסרלאוף היחידה למחלות זיהומיות המרכז הרפואי ע”ש סוראסקי, ת”א. The Common Cold The common cold is mild, self-limited, catarrhal syndrome. SIGNIFICANCE-

E N D
Respiratory Tract InfectionsCommon coldAcute and chronic bronchitisPneumonia (CAP and VAP) דר רות אורני-וסרלאוף היחידה למחלות זיהומיות המרכז הרפואי ע”ש סוראסקי, ת”א
The Common Cold The common cold is mild, self-limited, catarrhal syndrome • SIGNIFICANCE- • The leading cause of acute morbidity and of visits to a physician. • Major cause of school and industrial absenteeism.
ETIOLOGY • Five families of viruses: • Myxovirus, • Paramyxovirus, • Adenovirus, • Picornavirus • Coronavirus Adenovirus
VIRUSES ASSOCIATED WITH COMMON COLD • Antigenic type%of cases • Rhinoviruses 100 types +1 subtype 30-40 • Coronavirus 3 or more types > 10 . • Parainfluenza virus 4 types • Respiratory syncytial virus 2 types • Influenza virus 3 types 10-15 • Adenovirus 47 types 5 . • Other viruses (Enterov., Rubella, 5 • Rubeola, Varicella) • Presumed undiscovered viruses 25-30 • Group A b-hemolytic streptococci 5-10.
DISTRIBUTION- worldwide SEASONAL INCIDENCE- Colder month of the year, or rainy season in the tropics. ATTACK RATES- During the season Adults have 6-8 colds/ 1000 people/ day. (Children 9/1000) In the summer Adults have 2-3 colds/ 1000 people/ day.
TRANSMISSION- Close contact (direct contact with infectious secretions or aerosol with large and small droplets) PATHGENESIS- viral infection of mucous membrane of nose, sinuses, throat and ear.
CLINICAL CHARACTERISTICS- Incubation – 24-72 hours Nasal discharge and obstruction, sneezing, soar or scrachy throat and cough. Low fever in adult, higher in children. Max. severity during the 2nd or 3rd day. Median duration – 1 week but in ¼ the disease last 2 weeks.
DIAGNOSIS- • Clinical • Laboratory • TREATMENT- • TLC, decongestants, cough control, worm saline gargles. • PROSPECT OF NEW TREATMENT- • Antiviral treatment • Virucidal hand wash • Preventive treatment
ACUTE BRONCHITIS • Acute inflammation of the tracheo-bronchial tree, associated with generalized respiratory infection
ETIOLOGY Respiratory viruses – Mild disease with Rhinoviruses and some Coronaviruses, and more sever disease with Influenza virus and Adenovirus and lately with SARS (an new emerging Coronavirus.) Respiratory bacteria – Bordetella pertussis, Mycoplasma pneumoniae, Chlamydia pneumoniae.
VIRUSES ASSOCIATED WITH ACUTE BRONCHITIS and cough • %Of cases • Influenza 75-93 • Adenovirus 45-90 • Renoviruses 32-60 • Coronaviruses 10-50 • RSV 61 • Coxsackieviruses 26 • Parainfluenza virus 2-45
DISTRIBUTION- worldwide SEASONAL INCIDENCE- all year, more cases in the winter, epidemic. ATTACK RATES- in the UK: Mean 40-50 / 100,000 people Winter 117-170 / 100,000 Summer 26-42 / 100,000
TRANSMISSION- Close contact (direct contact with infectious secretions or aerosol with large and small droplets) PATH0GENESIS- Hyperemia and edema of the tracheobronchial mucous membrane and increase in bronchial secretions. Local – extensive distraction of the airway epithelium. Slow down of bronchial tree mucociliary function. May play a role in pathogenesis of chronic obstructive lung disease.
CLINICAL CHARACTERISTICS- • Cough begins early and tends to become more prominent as the illness progresses. • The cough can continue for 2-3 and even more weeks depend on the causing organism. (If the cough takes longer look for chronic disease) • Nasal discharge and obstruction, sneezing, soar or scratchy throat for 3-5 days
DIAGNOSIS- clinical diagnosis is suspected with any acute RTI with cough. R/O pneumonia (history, exposure, physical examination and if needed chest x-ray). Specific cultures. TREATMENT- Symptomatic- to control the cough (cough suppression and hydration) Antibacterial or antiviral therapy: according to the causing organism. PREVENTION- vaccination and medications
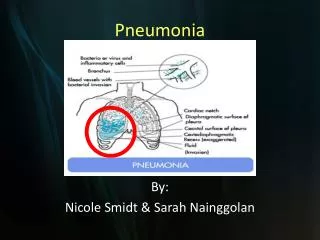
COMMUNITY ACQUIRED PNEUMONIA (CAP) דלקת ראות מוגדרת כתהליך דלקתי ריאתי עם קונסולידציה של רקמת הראה עקב גורם זיהומי.
DISTRIBUTION- worldwide -ATTACK RATES במי פוגעת דלקת הריאות בקהילה ? בכל אחד !!! -בשכיחות של 12 חולים ל- 1000 תושבים לשנה בחתך אוכלוסיה לפי גיל- • AGE FREQUENCY / 1000 • 35 – 44 0.54 • > 65 11.6 • nursing home residents 33
ETIOLOGY מי גורם לדלקת הראות בקהילה ? בשנות ה- 30 מרבית דלקות הראה (כ- %80) נגרמו ע"יStreptococcus pneumoniae היום : למרות מאמצים לזיהוי הפאתוגן, לפחות במחצית (%50) מהמקרים שמתאשפזים, נשאר הגורם לא ידוע. תוצאות נסיונות לזיהוי נמרץ של הפאתוגן כוללTransthorcic aspiration, Thoracocentesis or Bronchoscopy 43%- Unknown 8%- Polymicrobial 49%- One Pathogen
גורם לדלקת ראות בסדרות שונות: • THE ORGANISM % OF THE CASES • Unknown 25 – 45 • Strep.pneumoniae 14 - 28 • Haemophilus influenzae 0 – 12 • Legionella sp. 10 – 14 • Mycoplasma pneumoniae 5 - 7 • Infuenza virus 0 - 5 • Staph. aureus 1 - 3 • Strep. sp 0 – 3 • Chlamydia pneumoniae • C. psittaci 0 - 4 • Aerobic gram negative bacilli 3 - 12
PNEUNOMIA COUSING ORGANISMS • BACTERIA ATYPICAL BAC. • S. pneumoniae K. pneumoniae M. pneumoniae • H. influenza E. coli L. pneumophila • M. catharalis P. aeruginosa C. pneumoniae • S. aureus C. psitaci • Strep. sp. C. burnetii • OTHERS ANAEROBES FUNGI • F. tularensis P. jerovicii (PCP) • Nocardia sp. Aspergillus sp • Staph. Epidermidis • Myc. tuberculosis
CLINICAL CHARACTERISTICS- קליניקה טיפוסית:חום, צמרמורת, כאב פלאוריטי, שעול פרודוקטיבי עם כיח מוגלתי קליניקה לא טיפוסית: מהלך סוב-קליני, שעול לא פרודוקטיבי או שעול פרודוקטיבי עם כיח מוקואידי. • בהשוואה של הסימפטומים בדלקת ראות מגורם טיפוסי ולא טיפוסי לא נמצאו הבדלים משמעותיים) • במבוגרים:פחות סימפטומים ראתיים (שיעול), +/- חום, +/-בלבול • בחולים מדוכאי חיסון:סימפטומים לא טיפוסיים • ומחוללים לא שיגרתיים ( אופורטוניסטים)
DIAGNOSIS- • צלום חזה נחשב ל - “ GOLD STANDARD ” לאבחנה של דלקת ראות. • ** אי - אפשר לעשות אבחנה מיקרוביולוגית על סמך צלום רנטגן.
דלקת ראות לוברית (LOBAR PNEUMONIA)
קוורנה שחפתית בפסגת ראה ימנית
דלקת ראות עם תסנינים דו-צדדים BILATERAL INFILTRATES
דלקת ראות דו-צדדית קשה
אבחנה בטוחה • חיידק פאתוגני בתרבית דם. • חיידק פאתוגני בתרבית מנוזל פלאורלי. • נוכחותPneumocystis carinii במשטח כיח אוBAL. • עליה פי 4 בנוגדנים ל- Mycoplasma pneumoniae. • עליה בכיל נוגדנים פי 4 לפחות או בידודLegionella • נוכחות אנטיגן ליגיונלה בשתן. • אנטיגן בסרום או בשתן ל- Strep. Pneumoniae.
אבחנה אפשרית • צמיחה בינונית עד רבה של חיידק פאתוגני דומיננטי בתרבית כיח כאשר המשטח הישיר מתאים לאבחנה. • צמיחה דלה של חיידק פאתוגני בתרבית כיח וצביעת גרם מתאימה בתלות בחיידק.
מכשולים בדרך לאבחנה • כ- %30 מהחולים אינם יכולים לתת דגימת כיח. • כ- %30 מהחולים קיבלו אנטיביוטיקה לפני הפניה למיון. • כ- %25 מהמחוללים של דלקת הראות הם א-טיפים וקשים לאיבחון.
בדיקות לאבחנה • צילום חזה • בדיקת דם לגזים • ספירת דם • בדיקת דם לכימיה כולל אלקטרוליטים, תפקודי כליה וכבד. • תרביות דם • סרולוגיה ל- HIV • כיח למשטח ישיר ותרבית כולל למיקובקטריה. • נוזל פלאורלי עם יש – למשטח ישיר ותרבית, ספירת תאים, חלבון, גלוקוזpH, LDH. • טסטים ישירים: אימונופלואורסצנציה ואנטיגן לליגיונלה סרולוגיה למיקופלסמה.
גורמי סיכון למהלך מסובך של דלקת ראות או מוות בחולים עם CAP • גיל > 65 שנה • מחלת רקע שמחמירה בזמן דלקת ראות- IHD, CHF, : CRF, COLD. • מחלה ממאירה • מצב לאחר כריתת טחול • שינוי במצב ההכרה • אלכוהוליזם
טיפול אימונוסופרסיבי • קצב נשימה > 30 לדקה • ל.ד. דיאסטולי < 60 מ"מHg, ל.ד. סיסטולי< 90 מ"מHg. • היפונתרמיה • רמת קריאטינין > 150mM / L, רמתBUN > 7mM / L. • 30,000 > WBC > 3,000 למיקרוליטר. • Po2< 60mmHg אוPco2> 48mmHg כשהחולה נושם באויר החדר.
רמת אלבומין < 30 g/L • רמת המוגלובין < 9 g/L • S. aureus אוP. aeruginosa כמחולל דלקתהראות. • בקטרמיה • ממצא מולטי- לוברי בצלום חזה. • התקדמות מהירה של התהליך הדלקתי בצילוםחזה (> 50% תוך 36שעות).
טיפול • א. טיפול אנטי-מיקרוביאלי • כנגד חיידקים • כנגד וירוסים • כנגד פטריות • כנגד טפילים • ב. טיפול תומך • מתן נוזלים, הנשמה, שמירה על ש”מ אלקטרוליטים • פיסיוטרפיה נשימתית וכד’ • ג. טיפול מונע • חיסונים, אימונוגלובולינים, אנטיביוטיקה .
דוגמה לטיפול בחולה דלקת ראות אמבולטורי : Doxicyclin, Macrolides, New Quinolones דוגמה לטיפול בחולה דלקת ראות אמבולטורי קשה : 2nd or 3rd generation Cephalosporin iv + one of the above דוגמה לטיפול בחולה עם דלקת ראות קשה בטיפול נמרץ : 4th generation cephalosporin iv+ Quinolone iv +/-rifampin or carbapenem + new macrolide
NOSOCOMIAL PNEUMONIA includes Hospital acquired pneumonia Ventilator associated pneumonia
הגדרה דלקת ראות נרכשת (דר”נ) בבי”ח היא תהליך דלקתי- זיהומי של רקמת הראה, שהחל 72 שעות או יותר לאחר אשפוז.
נתונים • דר”נ היא הזיהום שנרכש בבי”ח (נוזוקומיאלי), • השני בשכיחותו • דר”נ מהווה % 18-13 מסך הזיהומים הנרכשים • בביה”ח. • דר”נ היא סיבת המוות השכיחה ביותר בחולים • מאושפזים ומהווה %27-33. • התמותה גדולה יותר בחולים בקטרמיים או • בזיהומים עם פסוידומונס או אצינטובקטר.
התחלואה הגבוהה הקשורה לדר”נ כוללת • אשפוז ממושך (7-9 ימים בממוצע) ומחיר גבוה • למערכת • (בארה”ב מעריכים את ההוצאה ב-2בליון דולר בשנה)
גורמי סיכון לחלות בדר”נ קשורים ל: א. מצבו של החולה ב. Infection control ג. פעולה פולשנית ד. אחרים
גורמי סיכון לחלות בדר”נ קשורים ל: • א.מצבו של החולה • גיל > 70 שנה • מחלות רקע קשות (ממאירויות) • מחלות שעלולות לגרום לתמותה במקבילכמוCOPD, אלכוהוליזם, א”ס כליות, פגיעה ב-CNS • תת-תזונה • אצידוזיס מטבולית • סינוסיטיס
גורמי סיכון לחלות בדר”נ קשורים ל: • א. מצבו של החולה (המשך) • חסר הכרה • חסר רפלקסים של דרכי האויר (שעול, בליעה) • מחלות נוירומוסקולריות • חבלת ראש
גורמי סיכון לחלות בדר”נ קשורים ל: • ב. Infection control • אי- רחיצת ידיים • מיעוט בלבישת חלוקים והחלפת כפפות • שימוש בציוד הנשמה מזוהם
גורמי סיכון לחלות בדר”נ קשורים ל: • ג. פעולה פולשנית • כל הגורמים הקשורים להתערבות פולשנית- • כל הפעולות שמורידות את איכות ההגנה הטבעית ומאפשרות חדירת כמות גדולה של חיידקים.
דוגמאות: 1. תרופות • חומרי הרדמה, נרקוטיקה- עלולים להגביר אספירציה • סטרואידים, ציטוטוקסיקה- מורידים רמת חיסון • אנטיביוטיקה מתקדמת- מעלה שכיחות זיהומים , בחיידקים יציבים • תרופות סותרות חומצה ו- H2 Blocker - מעלה כמות • חיידקים בקיבה וסיכון מוגבר לדר”נ בחולה מונשם • מהמקרים מדובר באותם חיידקים )55%)
דוגמאות: 2. מכשירים • טובוס - הנשמה מגבירה סיכון לדר”נ פי 20 בהשוואה לחולה לא מונשם. קיים סיכון של %1-3 יומי לחלות בדר”נ, במקרה זה נקראת גם VAP- Ventilator Associated Pneumonia • זונדה נאזו-גאסטרית • ברונכוסקופיה
גורמי סיכון לחלות בדר”נ קשורים ל: • ד. אחרים: • ניתוח באזור בית חזה או בטן עליונה • משך הניתוח • משך האישפוז • אספירציה
מי החיידקים הגורמים לדר”נ ? • Streptococcus pneumoniae - 5-20% • Haemophilus influenzae - 5-15% • Staphylococcus aureus - 20-40% • Pseudomonas aeruginosa • E. coli • Enterobacter spp. - 25-60% • Klebsiella pneumoniae • Serattia marcescens • Acinetobacter
מי עוד ? • Legionella pneumopila - 0-5% • Mycobacterium tuberculosis - <1% • Anaerobes - <35% • Polymicrobial - 25-46% • VIRAL- RSV, Influenza, parainfluenza