Discriminative Questionnaire for Movement Disorders Diagnosis
This research presents a structured questionnaire to differentiate between psychogenic and neurogenic movement disorders, with efficient risk factor identification. The questionnaire demonstrates high specificity and utility, aiding in accurate diagnosis.

Discriminative Questionnaire for Movement Disorders Diagnosis
E N D
Presentation Transcript
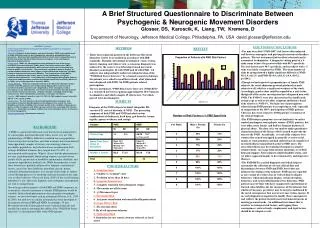
A Brief Structured Questionnaire to Discriminate Between Psychogenic & Neurogenic Movement DisordersGlosser, DS, Karoscik, K, Liang, TW, Kremens, D  Department of Neurology, Jefferson Medical College, Philadelphia, PA, USA david.glosser@jefferson.edu DISCUSSION/CONCLUSIONS • The nine described “PMD-RFI” risk factors discriminated well between neurogenic and psychogenic movement disorders patients. The test instrument had excellent selectivity and is economical to administer. A diagnostic cutting point of > 4 risks seems to have the greatest utility with 88% specificity. Five risk factors gave 96% specificity, and no subject with > 5 risks was falsely categorized as PMD. The mean number of risks by group showed a highly significant difference (NMD M=1.9; sd=1.9, and PMD M=4.8; sd=1.8, t=4.4, df=32; p<.0001). • Though we had expected a preponderance of female PMD subjects, the serial admission protocol produced no male subjects at all; which is a significant weakness of the study. Accordingly, gender alone could be regarded as a risk factor; though all of the senior investigators have diagnosed men with PMD. The PMD S’s were also characterized by significantly younger age as well as the other symptom and history-based risks relative to NMD S’s. The high rate of participation refusal among PMD patients was surprising as well; especially in comparison of the 100% participation of NMD patients. This may have been related to PMD patients’ resentment of the clinical diagnosis. • The PMD subject group bore several similarities to earlier studied psychogenic non-epileptic seizure (PNES) patients, but were older, more female, and had less frequent histories of physical abuse. The data set is too small to make quantitative characterizations of the factors which seemed to provoke the onset of the PMD. Anecdotally, several of the subjects were women who seemed entrapped in generally aversive social, family, or work situations and had suffered one of a number of unrelated illnesses immediately prior to PMD onset. The antecedent illness may have produced temporary negative reinforcement, via escape from noxious situations, or yielded help and support. Some subjects sought disability status, and yet others appeared mainly to have had anxiety and depressive illnesses. • The PMD-RFI is a useful diagnostic tool which helps to systematize the collection of relevant clinical data and discriminates between NMD and PMD, but it does not delineate the etiology of the behavior. PMD may be regarded as one variant of a wider class of evolved distress display behaviors; which include pain display, certain deception behaviors, and social subordination stress behaviors. PMD patients may be those who have exaggerated constitutional or learned vulnerabilities for the emergence of the behavior, but whether it becomes persistent may be largely conditioned by the social consequences that accrue to it once it does emerge. If so, early diagnosis is important to modify those consequences and redirect the patient towards more instrumental means of meeting personal needs. An additional instrument that is sensitive to etiological risk factors, and tapping those consequences; such as family, employment, and legal factors should be developed as well. METHODS • Thirty four sequential patients of the Jefferson Movement Disorders Center were enrolled in accordance with IRB standards. Through conventional neurological exam, testing, history, imaging, and video review, a consensus diagnosis was achieved by the center’s two fellowship trained movement disorders neurologists; 24 with NMD and 10 with PMD. All subjects also independently underwent administration of the “PMD Risk Factor Interview” by a trained research technician. Six patients were asked to enroll but refused; all of whom had been diagnosed with PMD. No NMD patients refused participation. • The test instrument, “PMD Risk Factor Interview (PMD-RFI)” is a structured interview requiring approximately 10-15 minutes to administer and which samples 15 risk factors; 9 of which proved to be discriminative. SUBJECTS Diagnoses of the NMD subjects included: idiopathic PD, vascular PD, cervical dystonia, & NPH. The presenting symptoms of both PMD and NMD included various combinations of dyskinesia, head drop, gait disorder, tremor, rigidity, spasm, weakness, and vertigo. RESULTS ABSTRACT (revised) • A brief structured interview to discriminate between psychogenic & neurogenic movement disorders. • Objective: Diagnosis of psychogenic movement disorders (PMD) is principally based on exam and history and can be challenging for specialists and bewildering for generalists. We present data regarding the utility of a brief structured questionnaire to identify risk factors that discriminate between neurogenic versus psychogenic movement disorder patients. • Background:PMD’s are stereotyped behaviors attributed to one of the known neurogenic movement disorders (NMD); when in fact this is not the case. PMD’s represent diagnostic misattributions which have the social effect of transforming a behavior pattern into a disease. They can best be regarded as distress displays, or escape/avoidance behaviors which trigger culturally determined responses; including extensive medical interventions and disability. The symptoms can mimic NMD’s including: pathological gait, tremor, speech, speed, coordination, or atypical undifferentiated movements. In the related area of Psychogenic Non-epileptic Seizures, a risk factor model has shown excellent discriminative selectivity/sensitivity (Glosser,et al., 2008), and a similar approach is tested for PMD’s. • Design/Methods:Thirty four sequential referrals to the Movement Disorders Center, enrolled under IRB approval, were independently diagnosed by consensus of 2 movement disorders specialists and categorized as either neurogenic (n=24) or psychogenic (n=10). Subsequently, a 15 minute structured interview was administered by a research technician assessing: symptom evolution, semiology, medico-legal, substance use, other somatizations, psychiatric, and trauma risk factors. • Results:NMD subjects’ mean # of risks =1.9; SD=1.8. PMD subjects’ mean # risks =4.8; SD=1.8. t=4.4, df=32; p<.0001. • Conclusions: The test instrument discriminated well between neurogenic and psychogenic movement disorder patients. Early diagnosis may reduce the social disability, psychiatric morbidity, and economic burden of the condition. Expansion to a greater number of subjects, with follow-up may reveal factors associated with outcome differences. Examination of subject variables may reveal etiological factors of relevance to clinical management. • Study Supported by:Departmental resources Number of Risk Factors x % PMD Specificity BACKGROUND A PMD is a persistent behavioral event that has been interpreted to be a neurogenic movement disorder when, in fact, it is not. The epidemiology of PMD is difficult to establish since no population based surveys have been done, and other estimates have been derived from opportunity samples of tertiary care neurology clinics or psychiatric populations, and selection biases are inherent in both settings. Published estimates have ranged from 9%-60% of movement disorders patients. What is clear is that the phenomenon is not rare, is predominantly found among women, occasions lower quality of life, greater risk of morbidity and mortality, disability, and expensive unproductive medical care. While the propensity to emit these behaviors is probably influenced by inherent constitutional factors, once it has been labeled as neurologic disease, potent culturally determined responses to it emerge which shape its further course through processes of modeling and reinforcement in the same way as other behaviors (Glosser & Stern, 2000). If the social learning hypothesis is true, then early diagnosis and contingency management are vital to mitigate harm. Given the great heterogeneity of both PMD and NMD symptoms, an economical, selective instrument to identify PMD patients would be valuable. In the related phenomenon of psychogenic non-epileptic seizures, we have developed such an instrument (Glosser, et al., 2003 & 2008), but until now no similar instrument has been developed to discriminate between PMD and NMD. Accordingly, 34 new Movement Disorder Center patients were evaluated clinically and enrolled in a study to determine the ability of the “PMD Risk Factor Interview” to discriminate PMD from NMD patients. PMD RISK FACTORS • A. Symptom Onset • 1. “Sudden vs. Gradual” onset • 2. Evolution in less than 14 days • B. Symptom Inconsistency • 3. Complete remission with subsequent relapse • 4. Movements not all the same • 5. >3 Movement types • C. Psychiatric Risk • 6. Any prior consultation with mental health professional • D. Abuse History Risk • 7. Hx of sexual abuse • 8. Hx of self-injurious behavior • E. Medicolegal Risk • 9. Sued other for any reason, attorney referred, or hx of arrest