Download
1 / 37
370 likes | 508 Views
ILLNESSES OF SALIVARY GLANDS, LIPS, TONGUE & MOUTH CAVITY. Associate-prof. V.Voloshyn. According prof. Pospishil O.V. & prof. Strukov A.I. ILLNESSES OF SALIVARY GLANDS. innate ( congenital): agenesia , hypogenesia, octopia, hypertrophy of glands, additional glands ;

E N D
ILLNESSES OF SALIVARY GLANDS, LIPS, TONGUE & MOUTH CAVITY Associate-prof. V.Voloshyn According prof. Pospishil O.V.& prof. Strukov A.I.
ILLNESSES OF SALIVARY GLANDS • innate (congenital): • agenesia, hypogenesia, octopia, hypertrophy of glands, additional glands; • imperforation of channels, narrowing or atresia, anomalous branches out, defects of walls with formation of fistulas; • acquired: • sialoadenitis, sialoalitiasis, cysts, tumours and tumular processes. 2
Sialoadenitis classification (A) • primary (independent disease); • secondary (complication or displays of other disease) • (B) • Acute; • Chronic; • Chronic with acuting 3
Etiology of Sialoadenitis • Microbes • Viruses • Autoimmune process 4
EPIDEMICPAROTITIS RNA virus – mixovirus group
CYTOMEGALIA owl eye DNA virus – herpes group
Sjogren’s disease AUTOIMMUNE SIALOADENITIS Mikulich’s disease • dry keratoconjunctivitis; • xerostomia; • rheumatic arthritis. • xerostomia; • xerophtalmia.
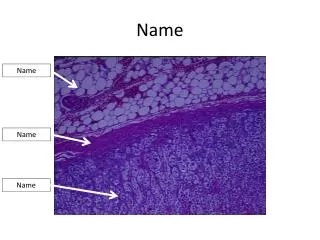
Pathoanatomyof Sialoadenitis • Acute sialoadenitis: • serosal, purulent (local or diffuse); • gangrenous; • Chronic sialoadenitis: • productive • intermediate 8
Purulant Sialoadenitis Chronic Sialoadenitis
Complication and consequencesof Sialoadenitis • Acute sialoadenitis→convalescence or chronic prss; • Chronic →sclerosis (cirrhosis) of gland with atrophy of acinus portion, stromal lipomatosis with the decline or function loss ; • →xerostomia. sclerosis of gland 10
SIALOLITHIASIS The concrements, whichpresent in a gland and more frequent in its channels are the basis of the disease. More frequently the stones appear in a submandibular gland; stones appear in parotid rarely; sublingual gland is almost never damaged. The men of middle ages ill mainly 11
Etiology and pathogeny. The gland channels dyskinesia, their inflammation, stagnation and saliva alkalining, increase of its viscidity, extraneous bodies penetration in the channels are the reasons of salivary stone formations. These factors are instrumental in falling out from saliva of the various salts (calcium phosphate, calcspar) with crystallization them on organic basis — matrix (ephithelial cells rejection, mucin) 12
Pathoanatomy. The formed stones have different sizes (from sands to 2 centimeters in a diameter), shapes (oval or oblong), colors (grey, yellow), consistencies (soft, densed). The acute inflammation (sialodochitis) appears at the channel obturation. Very often festering sialoadenitisdevelops. Sialoadenitis became chronic with the periodic acuteening afterwards. • Complication and consequences. The sclerosis (cirrhosis) of gland develops at chronic motion of sialoadenitis. 13
ADENOCELES • Adenoceles more often arise up in the small glands. The reasons of the cysts formations are trauma, channels inflammations with subsequent (послідуючим) sclerosis and obliteration. The sizes of cysts are different. Cysts with mucus or mucoid component are named mucocele. 14
TUMOURS • The tumours of salivary glands formed 6% in relation to all tumours which develop in a human; in stomatological oncology they make a greater particle (portion). 15
Classification of salivary glands tumors (World Health Protection Organozation): • Adenomas: pleomorphic (polymorphic), monomorphic (oxyphilic, adenolimphoma, other types). • Mucoepidermoid tumour. • Acinocell tumour. • Carcinoma: adenoceles, adenocarcinoma, epidermoid undifferentiated carcinoma in a polymorphic adenoma (the malignant mixed tumor). 16
Pleomorphic (polymorphic) adenoma: • is most widespread of salivary glands ephithelial tumours. Formed near 50% tumours of this localization. Almost 90% of cases they are in a parotid gland. Macroscopically: round or oval nodes, sometimes hilly, dense or elastic consistency, up to 5-6 cm in diameter. Tumor are surrounded by a thin capsule. The tissue is whitish, often with mucose and cysts. 17
Pleomorphic adoma Can be quite varied. Epithelial cells in the tumor may be rounded, polygonal, cubic, cylindrical and form as channel, solid fields, some nest tending.Cells of myoepithelium with light cytoplasm. Mucoid, mixoid and chondroid tissue areas. Hyalinosis, epidermidalization and keratosis present. 18
A monomorphic adenoma • is the bening tumour of salivary glands (1—3%); it is localized mainly in a parotid gland. A tumour grows slowly Histological classification: • oxyphilic; • adenolymphomas; • basal cells; • light cells; • mucoepidermal adenomas 19
Oxiphilic adenoma(onkocytomas) • Are formed by large cells with small grains in a cytoplasm. Localized mainly in the parotid glands. The cells are placed in a solid field. 20
ADENOLIMPHOMAS 8.2 8.3 21
A) THE MALIGNANT EPHITHELIAL TUMOURS OF SALIVARY GLANDS B) THE TUMULAR DISEASES-limphoepitelial defeat;-sialosis;-oncocytosis (at adults). 23
DISEASES OF LIPS, TOUNGE AND SOFT TISSUE OF MOUTH CAVITY • Cheilitis: • exfoliatic; • glandular; • contactic; • meteorological (actinic); • granulomatic (at Melcerson-Rosental syndrom); • Cheilitis of Manganotti; • inflammation of mouth corners; • furuncle of lips; • erysipelas (rose) 24
GLOSSITIS • desquamative glossitis; • diamond-shaped glossitis; • black pilose tongue; • chronic glossitis. 25
STOMATITIS(select next groups): • traumatic; • infectious; • allergic; • as a result of exogenous intoxications; • at somatic illnesses; • at dermatosiss 26
CANDIDALSTOMATITIS Tubular hyphens(9.3) 28
Pre-tumours changes • leuoplacy; • erytroplacy; • chailitis of Manganotti. 29
VILLOMA 32