Abdominal Exam for Advanced Practice
Abdominal Exam for Advanced Practice. CESAP/PACR 2012. Outline. History Risk Examination Abnormal Findings/Differential Diagnoses Variants for Children Variants for Elderly and Pregnancy. History. Presenting complaint Area, origin, pattern, duration, onset of symptom?

Abdominal Exam for Advanced Practice
E N D
Presentation Transcript
Abdominal Exam for Advanced Practice CESAP/PACR 2012
Outline • History • Risk • Examination • Abnormal Findings/Differential Diagnoses • Variants for Children • Variants for Elderly and Pregnancy
History • Presenting complaint • Area, origin, pattern, duration, onset of symptom? • Associated Symptoms • Menstrual/Sexual History? • PMH (surgical history, medications) • Other (Nutrition, Diet, ETOH/Drugs, Stress, Travel)
GI/GU Specific • Pain/Discomfort • Urinary habits • Nausea/vomiting/diarrhoea • Bleeding • Anorexia • Gyn/Ob history • What else???????
Bowel habits • http://www.youtube.com/watch?v=jsVgi8hoFFc • Ask the patient about bowel movements • Frequency of the bowel movements • Consistency of the bowel movements (diarrhea vs. constipation) • Any pain with bowel movements • Any blood or black, tarry stool (meleana) with the bowel movement • Ask about the color of the stools (white or gray stools can indicate liver or gallbladder disease) • Look for any associated signs such as jaundice or icteric sclerae
Risk Factors • BMI (over or under?) • Health Behaviours (ETOH, Drugs, Crash Diets, Medications) • Chronic Disease • Modifiable (change in peristalsis?) • Non-Modifiable (medications, inactivity, family history)
Preparing for Exam • Stethoscope • Full exposure to abdomen however maintain appropriate draping • Have patient lie supine with arms at sides, legs slightly bent
Anatomy of the abdominal GI tract Landmarks Musculature Vasculature Vital Organs
Kidneys • Described as posterior organs • The upper poles are protected by ribs • Costovertebral angle/ Renal angle This is the angle formed by the 12th rib & transverse process of the upper lumber vertebrae.
Pain in Abdominal Areas Types of Visceral Pain
History Taking of Problems of the Abdomen: GI Tract • Qualify the patient’s pain • Visceral pain: when hollow organs (stomach, colon) forcefully contract or become distended. Solid organs (liver, spleen) can also generate this type of pain when they swell against their capsules. Visceral pain is usually gnawing, cramping, or aching and is often difficult to localize (hepatitis) • Parietal pain: when there is inflammation from the hollow or solid organs that affect the parietal peritoneum. Parietal pain is more severe and is usually easily localized (appendicitis) • Referred pain: originates at different sites but shares innervation from the same spinal level (gallbladder pain in the shoulder)
Review of Systems-Tips • Remember these are subjective findings you ask the patient • Questions often pertain to symptoms but also to common diseases related to the system you are examining • Start with a generic question “How is your digestion?” or “How about your bowels?” • The goal is to uncover problems the patient may have overlooked.
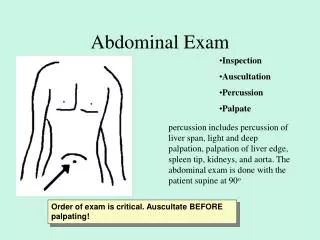
Examination • Inspection • Auscultation • Palpation • Percussion
Examination • Consider landmarks • Four quadrants/ Nine regions • 1. Epigastric, 2.Umbilical, 3.Suprapubic, 4&5.Right and Left hypochandriac, • 6&7. lumbar • 8&9. inguinal areas
Systemic Inspection • Inspection should include looking for signs of chronic disease overall: • Nail beds/palms of hands • Skin/hair • mucous membranes (mouth and anus) • eyes
Focused Inspection • Contour of abdomen- • Rounded? Protuberant? Scaphoid? Flat? • Skin characteristics- • lesions, hernia, scars, striae, tattoos, echymosis, hair distribution • Other • gravid, ascites, nodules • Aortic pulsations, peristalsis, movement, vein visibility
Palpation • One or two handed technique. Use finger pads not tips • Watch facial expressions! • Palpate in three phases: light, deep and during respiration • Light for tenderness. • Deep palpation of organs and to detect masses/tenderness. • Palpate during respiration to feel for “shifting” of organs with breathing.
Palpation • Assess organs, muscle spasms, masses, fluids and tenderness (6 F’s) • Check umbilical ring (round and no abnormalities)
Palpation of Liver Palapation of the liver should be performed by placing your hand on the right upper quadrant, with index finger in line with the costal angle. Ask patient to breath in and push hand inwards and upwards. A liver edge should be felt.
Palpation of the kidneys To examine the kidneys place hand on right side of abdomen below the costal margin, above the umbilicus and the left hand under the back below the liver. Press firmly up with the left hand and down with right. Repeat on the left hand side. If enlarged the kidney will be palpable.
Renal angle • Percuss the renal angle with your fist with moderate force.
Palpating the Spleen A spleen is not palpable unless it is enlarged. Use your left hand under left lower rib cage, position finger tips so they point to axilla and press inwards and upwards. You can also ask the patient to take a deep breath and feel again.
Abdominal Reflexes • Lightly but briskly stroke each side of the abdomen using a key or tip of wooden applicator (Tests T8-10 (above the umbilicus) and T10-12 (below the umbilicus) • Note the contraction of the abdominal muscles and the deviation of the umbilicus towards the stimulus • If reflex diminished could be related to obesity or pregnancy
Percussion • Systematic route • To assess size and density of organs • To distinguish gas, ascites, cystic or solid masses • Tympany= air. Usually high pitched/musical • Dullness=organs or masses. Short, high-pitched with little resonance.
Percussion of liver • When percussing the liver you are measuring it’s size, start at the right mid-clavicular line where you will start with lung resonance and percuss down the sound changes to dullness. Then percuss up starting in the mid clavicular line level with umbulicius and note where the sound changes. Measure between these two points .
Percussion of Liver • Important to define borders, especially in diseased patient • Normal measurement 6-12cm in adult • Check for nodules, tenderness, irregularities • Report liver size via span and extent of projection from costal margin.
Percussion of Spleen • Percuss for dullness as usually tympanic! (so if hear dullness (+) finding!) • Typically from 6th to 10th rib • Have patient inspire while percussing….if spleen enlarged, tympany changes to dullness
Percussion • Abnormal findings
Auscultation • Use diaphragm for bowel sounds • Use bell for vasculature sounds…bruits, friction rubs, venous hum • Listen for clicks/gurgles: “borborygmi”…5-35 per minute. Usually more active after meal. • Absence of sounds established only after 3 minutes of continuous listening. • *Should be done prior to percussion/palpation as bowel sounds may change with manipulation
Auscultation • Absent bowel sounds indicate ileus • Increased bowel sounds (including high-pitched tinkling or marked borborygmi) indicate obstruction, bleed, malabsorption, carcinoid syndrome
Abnormal Findings/Differential Diagnoses • Cholecystitis….+ Murphy sign (cessation of inspiration with palpitation of gallbladder.) • Pancreatitis, epigastric tenderness or ectopic pregnancy, +Cullen sign (ecchymosis around umbilicus.) • Alcoholic Hepatitis…palpate an enlarged liver with marked tenderness • Dysphagia....complaint of pain in the throat or chest region indicates oesophageal disorder.
Abnormal Findings/Differential Diagnoses • Costovertebral angles for kidney tenderness…indicates renal disease/pyleonephritis • Suprapubic tenderness typical with cystitis • Ascities…percuss for shifting dullness and/or test for fluid wave (often found too late) • Appendicitis….check for rebound tenderness (Romberg sign), guarding, McBurney’s sign, Psoas sign, Obturator sign
Risk Factors • Health Behaviours (ETOH, Drugs, Crash Diets, Medications) • Chronic Disease • Modifiable (Drugs, depression, stress, inactivity) • Non-Modifiable (medications, neurologic disorders, family history)
Anus, Rectum and Prostate • Terminal portions of GI tract • Sphincter/ring muscles internally and externally in anus • Mucosal tissue • Anus controls excretion of faeces, rectum stores it • Rectum continuous with sigmoid colon • Prostate located at base of bladder/surrounds the urethra. Composed of muscular and glandular tissues. Responsible for secretion
Review History • Change in patterns, consistency, colour, odour, flatus, pain, nausea, fever, distension, change in urinary function, hesitancy, nocuturia, dysuria, dripping/dribbling, urethral discharge? • For exam…….consider patient position…side lying, knee-chest, standing…or perform during pelvic