Download
1 / 16
160 likes | 603 Views
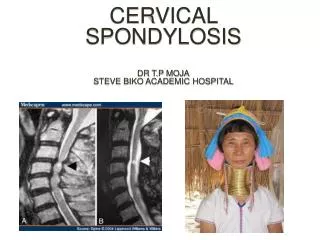
CERVICAL SPONDYLOSIS DR T.P MOJA STEVE BIKO ACADEMIC HOSPITAL. Pathophysiology. Disc degeneration -nucleus pulposus loses water content, fissuring, loss of height and bulging annulus. -acute rupture and herniation may occur Secondary changes due to increased and uneven loading of forces

E N D
Pathophysiology • Disc degeneration -nucleus pulposus loses water content, fissuring, loss of height and bulging annulus. -acute rupture and herniation may occur • Secondary changes due to increased and uneven loading of forces - Vertebral osteophytes - Facet and uncovertebral joint osteoarthritis and hypertrophy - Ligamentumflavum becomes thickened and may ossify - Spine deformity due to segmental instability Degenerative spondylolistheses Degenerative kyphosis or scoliosis • Narrowing of the central canal, lateral recesses and foramina with subsequent neural and vascular compression
Clinical Presentation • Asymptomticwith incidental radiographic findings • Symptomatic - in most cases: onset is slow and insidious . However some cases may be acute eg hyperextension injury in minor trauma or acute disc herniation • Neck pain • Myelopathy • Radiculopathy
Neck pain • Occurs if there is a disc extrusion • Nerve root compression • Facet joint arthritis • Segmental instability • Often poorly localized • May radiate to the occipital region, shoulders, interscapular. • There may be associated stiffness of the neck from muscle spasm
Myelopathy • May be complex and variable • Most cases seem to present with a central cord syndrome, rarely brown squard, or complete myelopathy • Motor • -upper limbs: LMN Weakness • Clumsiness of the hands. Muscle wasting. Absent biceps reflex, inverted reflex, Triceps reflex may be brisk. Positive Hoffman reflex • -Lower limbs: Spasticity, difficulty walking. No or slight weakness. • Sphincters: usually no symptoms. Rarely mild bladder symptoms. ? Prostate
Sensory - No involvement - Patchy sensory loss - Paraesthesia in the hands, sometimes the feet and legs - May be asymmetrical or symmetrical - Different from radiculopathy in that it is not in a specific dermatomes - Lhermittes’s sign
Radiculopathy • May be acute if due to a disc protrusion • Slow and insidious if due to an osteophyte • Most common nerve root is C6 • Neck pain and shoulder pain. Pain radiates down the biceps, then the lateral aspect of the forearm then the thumb and index finger. • Head may be tilted to the affected side due to muscle spasm. Pain made worse by neck extension, relieved by neck flexion and shoulder abduction. • Often numbness, more often hand and fingers
Chronic cases – wasting and fasciculations of biceps and brachioradialis muscle. • Weakness of elbow flexion (Thumb-nose), and wrist extension. • Absent biceps and brachioradialis reflex
C5 nerve root radiculopathy • - Neck pain • - Shoulder pain, pain over the lateral aspect of the upper arm. • - Numbness or paraesthesia over the lateral aspect of the upper arm. • - Weakness of deltoid and biceps muscles, with absent biceps reflex • In severe cases, wasting of the deltoid and biceps muscles
Treatment • Neck Pain -Conservative -Rarely, surgery • Myelopathy -Surgery in most cases -Some may stabilize on conservative • Acute radiculopathy -Conservative -Surgery if indicated • Chronic radiculopathy -Most cases, surgery
Conservative treatment • Medication:Analgesia NSAIDS Diazepam Baclofen Carbamazepine, Gabapentin, Lyrica • Physiotherapy: Range of motion exercises Isometric exercises Heat and massage • Traction: Continuous or intermittent halter traction • Neck collar Soft neck collar < 1 week • Facet and Medial branch block – Cortisone, L.A, Radiofrequency
SURGERY • Anterior decompression • Anterior cervical discectomy and fusion • Corpectomy and fusion • Posterior decompression • Laminaplasty • Laminectomy