Download
1 / 44
540 likes | 2.17k Views
Injuries of the knee . By : Dr . Sanjeev. Varus and valgus. the alignment between two anatomical segments.

E N D
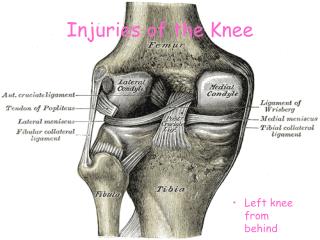
Injuries of the knee By : Dr . Sanjeev
Varus and valgus • the alignment between two anatomical segments. • To visualize the alignment, draw a line to illustrate the long axis of the proximal segment and another line to illustrate the long axis the distal segment. Compare the two lines, focusing on the the distal segment's alignmentwith respect to the proximal segment. In a valgus alignment, the distal segment deviates laterally with respect to the proximal segment. In a varus alignment, the distal segment deviates medially with respect to the proximal segment.
Knee ligament injuries • General principles • Aetiology • 1. Common ( athletes ): • Either direct due to the collision with another athlete or indirect due to rotation and twisting injuries • 2 . RTA • 3 . Fall from a height with twisting force
Mechanism of injury • 1 . Direct valgus ( bent outward ) force • 2 . Rotational or twisting force • Abduction ,Flexion and internal rotation of femur on tibia (Ab FIR): - causes damage to medial structures ,like tibial collateral , medial capsule , ACL , medial meniscus tear ``O donoghue unhappy traid ``:- medial collateral ligament injury + medial meniscus injury + ACL tear . Adduction , flexion and external rotation of femur on tibia ( Ad FER ) - causes damage to fibular collateral , lateral capsule , popliteus , iliotibial band , biceps , common peroneal nerve , anterior , posterial or both cruciates
Cont.. • 3. hyperextension force causes either ACL or PCL cruciate ligament injury . • 4 . Anteroposterior displacement (RTA) causes either ACL or PCL cruciate ligament injury .
Medial collateral ligament injury Clinical features : • Pain • Swelling • Haemarthrosis On examination : • Tenderness Stress test : A . Abduction or valgus stress test – positive B . Adduction or varus stress test – positive • To rule out the associated injuries , do anterior drawer test and lachman`s test
Investigation • Stress radiographs at 15 to 20 degree of valgus • MRI • Arthrograms and • Arthroscopy
. Arthroscopy (also called arthroscopic surgery) is a minimally invasivesurgical procedure in which an examination and sometimes treatment of damage of the interior of a joint is performed using an arthroscope, a type of endoscope that is inserted into the joint through a small incision. Arthroscopic procedures can be performed either to evaluate or to treat many orthopaedic conditions including torn floating cartilage, torn surface cartilage, ACL reconstruction, and damaged cartilage.
Arthrogram • An arthrogram is a test using X-rays to obtain a series of pictures of a joint after a contrast material (such as a dye, water, air, or a combination of these) has been injected into the joint. • This allows to see the soft tissue structures joint, such as tendons, ligaments, muscles, cartilage, and joint capsule. • These structures are not seen on a plain X-ray without contrast material. A special type of X-ray, called fluoroscopy, is used to take pictures of the joint. • An arthrogram is used to check a joint to find out what is causing symptoms or problem with joint. • An arthrogram may be more useful than a regular X-ray because it shows the surface of soft tissues lining the joint as well as the joint bones. • This test can be done on your hip, knee, ankle, shoulder, elbow, wrist, or jaw (temporomandibular joint)
Arthrogram Normal: • The joint capsule, the sac containing joint fluid, is normal. • The cartilage and other structures of the joint are normal. Abnormal: - there is a tear in the cartilage. - there is a tear in the ligaments or tendons of the joint. The tear may be partial or complete.
Classification of Ligament Injuries Tears of the medial collateral ligament are classified into first degree, second degree, third degree and third degree plus associated anterior cruciate ligament rupture
Classification 1st degree: • Definition : - small number of fibres torn • Pain : - slight • Swelling : - slight • Tenderness : - slight • Laxity : nil • Ability to work : - normal
Cont.. • 2nd degree : - • definition : - moderate number of fibres torn • Pain : moderate • Swelling : - moderate • Tenderness : - moderate • Laxity : - moderate • Ability to work : - with difficulty
Cont.. • 3rd degree : • Definition : - all fibres torn (i.e. complete rupture) • Pain : - variable • Swelling : - variable • Tenderness : - severe • Laxity : - severe • Ability to work : - unable
Knee Valgus Stress Test Indications • Evaluate for Knee Collateral Ligament instability Patient Position • Patient lies supine on table • Lower thigh rests on table edge, leg hangs off table Technique • Perform each stress in two positions • Knee in 0 degrees (full extension) • Knee stabilized by PCL and bony articulation • Knee in 30 degrees of flexion • Isolates collateral ligament for evaluation • Stabilize lower thigh with one hand • Apply gentle stress at patient's ankle or foot • Valgus stress tests medial collateral ligament • Varus stress tests lateral collateral ligament
Cont.. Precautions: Varus Stress Test • Varus Stress Test may give false positive result • Femur rolls externally if not supported • Slight knee flexion may allow for laxity • Interpretation: Positive Test implies Instability • See Ligamentous Sprain for laxity grading • Laxity on Varus stress suggests knee LCL Tear • Laxity on valgus stress suggests knee MCL Tear
Varus and valgus stress test. performed with the knee unflexed and at 30 degrees of flexion.
Treatment • Fresh injury : • 1st degree: symptomatic treatment , NSAIDs • 2nd degree : long leg cast for 4 – 6 weeks with knee in 30 to 40 degree of flexion • 3rd degree : surgical repair and brace for 4 to 7 months.
Anterior cruciate ligament (ACL) tear • Ligaments are strong, dense structures made of connective tissue that stabilize a joint. They connect bone to bone across the joint. • Function of the ACL: - - is to provide stability to the knee and - minimize stress across the knee joint: • It restrains excessive forward movement of the lower leg bone (the tibia) in relation to the thigh bone (the femur). • It limits rotational movements of the knee.
Mechanism of injury • External rotation with abductionof the knee or hyperextension of knee in internal rotation • 67 % of ACL tear is sports related
Symptoms of an acute ACL injury include - Feeling or hearing a pop in the knee at the time of injury. • Pain on the outside and back of the knee. • The knee swelling within the first few hours of the injury. This may be a sign of bleeding inside the knee joint. Swelling that occurs suddenly is usually a sign of a serious knee injury. • Limited knee movement because of pain or swelling or both. • The knee feeling unstable, buckling, or giving out. • After an acute injury, you will probably have to stop whatever you are doing because of the pain, but you may be able to walk.
Classification of ACL injuries Grade I sprain • The fibers of the ligament are stretched, but there is no tear. • little tenderness and swelling. • The knee does not feel unstable or give out during activity. Grade II sprain • The fibers of the ligament are partially torn. • little tenderness and moderate swelling. • The joint may feel unstable or give out during activity. Grade III sprain • The fibers of the ligament are completely torn (ruptured); the ligament itself has torn completely into two parts. • There is tenderness. • The ligament cannot control knee movements.
Differential diagnosis : haemarthrosis • Ligamentous tear (ACL ,PCL, etc.) • Osteochondral fracture • Peripheral meniscal tear • Capsular tear • Patellar dislocation • Intra – articular fracture ( commonest cause is ACL tear )
Clinical examination • Always examine the normal knee first and form a basis for comparision Clinical tests to diagnose ACL injury : • Lachman`s test • Anterior drawer`s test • Jerk test • Pivot shift test
The right hand grasps the tibia, in a position to pull it forward The position assumed for the Lachman test of the RIGHT knee The left hand holds the femur to stabilize it The right thumb is placed on the superior aspect of the tibia
The right hand then pulls the tibia foward to place the ACL under tension. The left hand lifts the femur slightly, such that the knee is in 30 degrees of flexion An exaggerated view of a positive Lachman test . As seen, the ACL (if intact) will resist anterior tibial translation
Grading of lachman`s test Value Interpretation 0 negative 1+ 0-5 mm of anterior displacement 2+ 5-10 mm of anterior displacement – . with no end point 3+ 10 mm of anterior displacement - . . with no end point
Anterior Drawer Test • used to detect Anterior Cruciate Ligament injury. • The patient is supine with knee flexed to 90 degrees and the tibia is grasped with observation of foreward translation of the tibia. • In acute injuries there may be significant pain and spasm so it is best to perform this test carefully the first time as subsequent tests will be less accurate. Compare the laxity with the opposite knee.
Jerk test • The patient's foot is wedged between the body and the elbow of the examiner • The examiner places one hand flat under the patient's tibia, pushing it forwards (force applied in an anterior direction), with the knee in extension • The other hand is placed against the patient's thigh, pushing the other way (force applied in a posterior direction) • The lower limb is taken into slight abduction, by the examiner's elbow, with the examiner's body acting as a fulcrum to produce the valgus • At 20°-30° flexion, pivot shifting will occur, lateral tibial condyle subluxates.
Pivot Shift • The test is performed by holding the heel in one hand, and applying a valgus stress, with the other hand behind the fibular head. • If you apply some anterior force as well as the valgus, the tibia subluxes easily. After the anterior subluxation of the tibia is noticed, the knee is slowly flexed, and the tibial will reduce with a snap at about 20-30º of flexion. This reduction can be augmented with an external rotation of the tibia, as noted in the photo. This is the 'pivot shift'..