Download
1 / 21
210 likes | 393 Views
PHM142 Fall 2013 Instructor: Dr. Jeffrey Henderson. Clinical Use of Coagulation Inhibitors. By: Jonathan Mak , Elsa Chien , Anna Guo PHM 142 – Biochemistry September 18 th , 2013. Introduction. Coagulation (Thrombogenesis) Process of clots formation (blood vessels)

E N D
PHM142 Fall 2013 Instructor: Dr. Jeffrey Henderson Clinical Use of Coagulation Inhibitors By: Jonathan Mak, Elsa Chien, Anna Guo PHM 142 – Biochemistry September 18th, 2013
Introduction • Coagulation (Thrombogenesis) Process of clots formation (blood vessels) Homeostasis (prevent blood loss) Use of platelet and fibrin-containing clots to stop bleeding Hemorrhage vs. Thrombosis
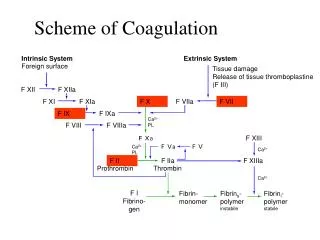
Physiology • Platelet Activation • Damage to endothelium • Exposure of collagen to circulating platelets • Extrinsic pathway (tissue factor pathway) • Intrinsic pathway (contact activation pathway) • Thrombin Activates • Factor XI • Factor VIII • Factor V • Factor XIII • Fibrinogen to Fibrin
Anticoagulants • Used to prevent cerebral and systemic emboli (blockage) in patients with: • acute myocardial infarction • valvular and non-valvular atrial fibrillation (arrhythmia) • prosthetic cardiac valves • Risk of excess bleeding • Most commonly used anticoagulants: warfarin, heparin
Vitamin K Antagonists • Reduce blood clotting by inhibiting vitamin K epoxide reductase • Therefore vitamin K epoxide cannot be reduced to the active form of vitamin K
Vitamin K Antagonists • 4 of 13 clotting factors require Vitamin K as a cofactor to undergo gamma carboxylation • When factors are not carboxylated, they cannot bind to the phospholipid membrane. The clot doesnt form. • Action can be reversed by administering vitamin K • avoid foods rich in vitamin K (i.e. leafy green vegetables such as kale and etc) • *remembering that vitamin K antagonists stop conversion of oxidized K epoxide to the reduced vitamin K • Teratogen can cause birth defects therefore contraindicated in pregnancy • Subgroups: • coumarins(i.e. warfarin) • Non coumarins (i.e. fluindione, phenidione)
Warfarin • Vitamin K Antagonist (VKA) • interferes with hepatic synthesis of coagulation factors II, VII, IX, and X and anticoagulant proteins C and S • Widely prescribed for prevention of stroke in patients with atrial fibrillation (53% reduction in risk with anticoagulation compared to aspirin and placebo group in patients with NVAF non valvular atrial fibrillation) • Narrow therapeutic index and thus requires routine monitoring • Dose determined by looking at: • Prothrombin time (PT): Time it takes for blood to clot after addition of a tissue factor. Normal PT without warfarin is usually 12-15 seconds • International normalized ratio (INR): mathematical manipulation of one’s PT based on a sensitivity standard accounting for differences in batches of tissue factor. Target INR 2.5. • Taken once daily • Peak effect 72-96 hours • Associated with multiple drug interactions like • Aspirin, Omeprazole and Cimetidine increase its effects • Penicillin and SSRI decrease its effects • Overdose: take vitamin K1 orally or parenterally
Quantitative Goals of PT/INR • Generally • INR = (PT test/PT normal) ^ ISI • ISI = value specific to tissue factor • INR= 2.0-3.0 (Generally people on the drug should be an INR of 2.0-3.0 for the purpose of thinning blood, but for people with artificial heart valves or with high risk of clot formation, an INR of 2.5-3.5 is used) • INR is used to adjust dose until the desired dose of medication is found. • INR < 2 generally results in thrombosis • INR >4.5 increased risk of bleeding • PT is measured both before use as a reference and then compared after the third day of anti-coagulant use. If there is a supratherapeutic indication, dose should be decreased. If stable, then more clinical tests are done over time to monitor any changes in PT. • PT of patient is compared against an average reference value based on people living in the area
Heparin • preparation of sulfated mucopolysaccharide injected IV or SC • Found in secretory granules of mast cells and released into vasculature at sites of tissue injury main purpose as defense instead of anticoagulation. • Two forms: unfractionated heparin and low molecular weight heparin (nadroparin) • Onset: rapid • Overdose: Take protamine sulfate • Risks: heparin induced thrombocytopenia 1% - 5% of patients receiving heparin • Type 1: heparin associated thrombocytopenia (HAT), early onset (within 48-72h) • Non immune cause of disorder • Does not cause an increased risk of thrombosis • Resolves itself after a few days • Type II (HIT): 5-10 days after • Associated with immune response and activation of platelets • High risk of thromboembolic events • Require direct thrombin inhibitors to prevent thrombosis
Unfractionated Heparin • 15000 daltons • Dosage: given frequently or as a continuous infusion (preferred). • Narrow therapeutic index and significant risk of bleeding • Indirect thrombin inhibitor that increases endogenous antithrombin activity
Unfractionated Heparin Mechanism of action • Heparin binds to thrombin via exosite 2. This heparin-thrombin complex then binds to antithrombin which activates antithrombin and induces a conformational change. This ultimately inactivates thrombin and other proteases involved with blood clotting such as factor Xa. The heparin-antithrombin complex inactivates activated coagulation factors II, VII, IX, X, XI, XII, kallikrein and plasmin
Low molecular weight heparin (nadroparin) • 3500 – 8000 daltons • Dosing: once or twice daily via deep subcutaneous injection • MoA: Through a conformational change in antithrombin III, it inhibits activated coagulation factor Xa • This is done more efficiently than the inhibition of thrombin (factor IIa) • This is why there are less side effects because factor Xa acts earlier in the coagulation cascade than thrombin
Direct Factor Xa inhibitors: Apixaban • Recommended dose is 5 mg twice daily; Taken Orally • Direct and highly selective active site inhibitor of Factor Xa. It does not require antithrombin III like heparin for AT activity. • Inhibits free and clot bound factor Xa and prothrombinase activity. • Indirectly inhibits platelet aggregation induced by thrombin • Contraindicated in patients with artificial heart valves
Direct Thrombin Inhibitor: Dabigatran • Orally active direct thrombin inhibitor DTI • Blocks conversion of fibrinogen into fibrin • Favored over warfarin for stroke prevention in patients with atrial fibrillation not caused by valvular problems • Contraindicated in patients with artificial heart valves • Onset: 2 hours • Dosage: 150 mg twice a day
Summary Slide • Coagulation is the process of blood clots formation, also known as thrombogenesis. It is used by the body to maintain hemostasis • Anticoagulants are used to prevent blood clots formation in patients with MI, arrhythmia, and prosthetic cardiac valves • Warfarin is a vitamin K antagonist (VKA) and interferes with hepatic synthesis of coagulation factors II, VII, IX, and X • Anticoagulant use is regularly monitored by the PT/INR test. INR levels are usually kept between 2.0 and 3.0. • INR<2.0 will likely result in thrombosis • INR>4.5 will likely result in excessive bleeding • Heparin is an indirect thrombin inhibitor which increases endogenous antithrombinactivity • Apixabanis a direct factor Xainhibitor • Dabigatranis a direct thrombin inhibitor.
Reference • Adam, S.S., McDuffie, J.R., Lachiewicz, P.F., Ortel, T.L., & Williams, J.W. (2013). Comparative effectiveness of new oral anticoagulants and standard thromboprophylaxis in patients having total hip or knew replacemnt: a systematic review. Annals of Internal Medicine, 159(4): 275-284. doi: 10.7326/0003-4819-159-4-201308200-00008 • Bounameaux, H. (1998). Unfractionated versus low-molecular-weight heparin in the treatment of venous thromboembolism. Vascular Medicine, 3 (41). Doi: 10.1177/1358836X9800300109 • Canadian Public Health Association (CPHA). (2012). Compendium of Pharmaceuticals and Specialties. Canada, 2012 edition. • Choudhury, A., Goyal, D., & Lip, G.Y.H. (2006). Ximelagatran. Drugs of Today, 42 (1). Pp. 3-19. ISSN 1699-3993. doi: 10.1358/dot.2006.42.1.893611 • Colman, R.W., Clowes, A.W., George, J.N., Goldhaber, S.Z., & Marder, V.J. eds. Overview of hemostasis. In: Hemostasis and Thrombosis: basic Principles and Clinical Practice, 5th edition. Philadelphia, Pa: JB Lippincott Co; 2006: 3-16 • Deloughery, T. (2013). Warfarin continuation was better than heparin bridging during pacemarker or ICD surgery. Annals of Internal Medicine, 159 (4): JC7. doi: 10.7326/0003-4819-159-4-201308200-02007 • Marlar R. & Saenko, E.L., (2013). Blood Coagulation & Fibrinolysis. WoltersKluwer Health. 24 (6), pp. 56 • O’Donnell, J. (2012). Anticoagulants: Therapeutics, Risks, and Toxicity – Special Emphasis on Heparin-Induced Thrombocytopenia (HIT). Journal of Pharmacy Practice, 25 (1). Pp. 22-29. doi: 10.1177/0897190011431146 • Pourrat, O., Neau, J.P., Pouget-Abadie, J.F., & Pierre, F. (2013). Thrombosis risk during pregnancy after history of cerebral venous thrombosis. Revue de Medecine Interne. pii: S0248-8663(13)00625-5. doi: 10.1016/j.revmed.2013.08.002 • Rabkin, M. Anticoagulation. Retrieved from http://www.medicineclinic.org/AmbulatorySyllabus4/NEW%20anticoagulation.htm