Download
1 / 14
140 likes | 270 Views
Worsening Racial Disparities in Access to Sellar and Parasellar Tumor Resection, 1988-2005. Debraj Mukherjee, M.D., M.P.H. Hasan A. Zaidi, B.S. Thomas Kosztowski, B.S. Kaisorn L. Chaichana, M.D. Roberto Salvatori, M.D. David C. Chang, Ph.D., M.P.H., M.B.A.

E N D
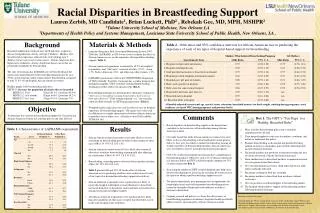
Worsening Racial Disparities in Access to Sellar and Parasellar Tumor Resection, 1988-2005 Debraj Mukherjee, M.D., M.P.H. Hasan A. Zaidi, B.S. Thomas Kosztowski, B.S. Kaisorn L. Chaichana, M.D. Roberto Salvatori, M.D. David C. Chang, Ph.D., M.P.H., M.B.A. Alfredo Quiñones-Hinojosa, M.D.
Hospital Caseload Volume Affects Surgical Outcome It has been well established in the literature that patients undergoing surgical intervention at high volume hospitals experience significantly reduced perioperative morbidity and mortality
Relationship between hospital or provider volume and major complications in neurosurgery • Transsphenoidal surgery for pituitary tumors in the United States, 1996–2000: mortality, morbidity, and the effects of hospital and surgeon volume. Fred G Barker II, Anne Klibanski, and Brooke Swearingen. Journal of Clinical Endocrinology and Metabolism 2003(88): 4709–4719. • Outcome and cost of craniotomy performed to treat tumors in regional academic referral centers. • Donlin Long, Toby Gordon, Helen Bowman, Anthony Etzel, Gregg Burleyson, Simone Betchen, Ira M. Garonzik, and Henry Brem. • Neurosurgery 2002(52): 1056-1063.
Methods • Use of the National Inpatient Sample (NIS) in-hospital discharge database for the years 1988-2005 • Contains discharge information from a stratified, random sample of 20% of all nonfederal hospitals in 37 participating states • Over 1,000 hospitals were sampled, with more than 7 million patient discharge records per year available in this database • Linked NIS to Area Resource File • Contains socioeconomic, environmental, and geographic characteristics
Databases • National Inpatient Sample (NIS) • 1988-2005 • Agency for Healthcare Research and Quality • ~7 million hospital stays from 1,000 hospitals per year • 20% stratified sample of US hospitals from up to 37 states • demographics, diagnoses, procedures • Area Resource File • (ARF) • 2004 • Health Resources and Services Administration • 6,000 data elements for each county within the US • SES, environmental, & geographic variables at the county level
Databases In order to link patient specific data from both the ARF and NIS, a common 5-digit state/county modified FIPS (Federal Information Processing Standards) code was utilized.
Inclusion / Exclusion Criteria Primary ICD-9 diagnosis code for a pituitary tumor: • 237.0 (neoplasm of uncertain behavior) • 194.3 (malignant neoplasm of the pituitary) • 227.3 (benign neoplasm of the pituitary) AND Primary ICD-9 procedure code for hypophysectomy: • 07.61 (partial excision, transfrontal approach) • 07.62 (partial excision, transsphenoidal approach) • 07.64 (total excision, transfrontal approach) • 07.65 (total excision, transsphenoidal approach)
Outcomes and Covariates • Primary outcomes were admission to a high-volume (>25 hypophysectomies/year) hospital or admission to a teaching hospital (Barker et al, 2003) • Covariates included patient-level, hospital-level, and environmental factors
21,717 pituitary tumor patients undergoing hypophysectomy, 1988-2005.
Patient characteristics and distribution across hospitals
Trends in admission of pituitary surgery patients to high-volume centers have steadily increased from 1988 to 2005
Multivariate analysis highlighting the odds of admission to high-volume hypophysectomy hospitals
Over an 18-year period, African–Americans, Hispanics and Asians exhibited progressively worse access to high-volume centers for hypophysectomy
Conclusions • A majority of patients undergoing neurosurgical intervention for pituitary tumors are being treated at low-volume centers. • Overall, more patients are being admitted to high-volume centers for neurosurgical intervention for pituitary tumors • Groups that continue to have relatively poor access to high-volume centers include: • Elderly patients • Low SES patients • Patients from areas with low neurosurgeon density • Disparities in access to care have worsened for blacks and Hispanics over the last two decades