Download
1 / 25
250 likes | 258 Views
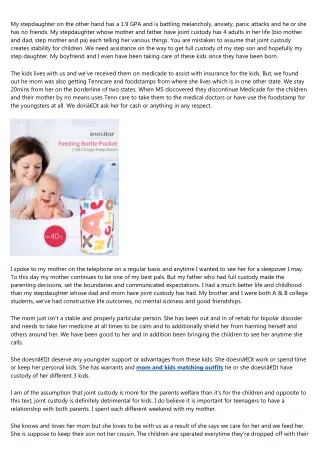
This report examines the effectiveness of house to house mobilization in measles SIAs in Africa, focusing on reaching marginalized populations. It includes case studies and data analysis.

E N D
HOUSE TO HOUSE MOBILIZATION FOR SUCCESSFUL MEASLES SIAs: SITREP AFTER FIVE YEARS IN AFRICA Bob Davis Measles/Health Delegate American Red Cross
WHOM DO WE HAVE TO REACH TO STOP MEASLES TRANSMISSION? • Ethno-linguistic minorities and slum dwellers • Marginalized and ‘floating’ populations, both urban, peri-urban, and rural • In a nutshell: Those who don’t watch CNN, don’t listen to the BBC, and don’t read the New York Times • Solution, for both polio and measles: next slide Photo, Prof. Stanley Foster
THE HOUSE TO HOUSE STRATEGY For GPEI, OPV SIA policy since 2001 PAHO policy in Latin America for measles SIAs: H2H mobilization in campaigns which vaccinated from fixed posts and fixed mobile posts H2H mobilization a best practice, UN supported measles SIA, Ethiopia, 2010 Used in Red Cross supported campaigns in 10 African countries: Benin, Burundi, C.A.R., Kenya, Mali, Mozambique, Namibia, Senegal, Tanzania, Uganda 2
COMMUNITY MONITORING AS PART OF H2H MOBILIZATION Wherever possible, line list the 9- to 59-month-olds in the week before the campaign, using RC volunteers, then trace defaulters after Day 1 of the campaign to bring them in from home. Example from Tanzania: 3
HOUSE TO HOUSE MOBILIZATION (cont.) Does H2H mobilization produce better results in measles SIAs? Probably: Traditional mass media approaches may miss the least readily accessible populations, even in urban areas. Herd immunity is more easily achievable when we systematically reach populations who lack, e.g., radio and TV. Data from 8 countries tend to support this hypothesis. 4
ADMINISTRATIVE COVERAGE ESTIMATES IN DISTRICTS WITH AND WITHOUT KENYA RED CROSS HOUSE TO HOUSE CANVASSING, 2009 MEASLES CAMPAIGN, NAIROBI
COMPARATIVE CAMPAIGN COVERAGE, NAMPULA PROVINCE, MOZAMBIQUE, 2008 Red Cross Districts Target 413,005 Vaccinated 401,604 Coverage 97.2% Others Target 214,481 Vaccinated 188,064 Coverage 87.7% 6
COMPARATIVE CAMPAIGN COVERAGE, BAMAKO, MALI, 2011 Red Cross Zones Target 660,000 Coverage 93.6% Others Do these percentages make a difference? Yes, when herd immunity starts at > 90% Target 210,317 Coverage 87.8% 7
RESULTS OF SITE INTERVIEWS WITH CAREGIVERS, TWO RURAL PROVINCES COVERED BY BURUNDI RC, 2012 SIA
ADMIN COVERAGE ESTIMATES, BURUNDI’S 2012 SIA, NATIONWIDE AND IN THE FOUR REGIONS WITH H2H MOBILIZATION
SOURCES OF INFORMATION CITED BY MOTHERS, ABOMEY, BENIN, SEPTEMBER 2011: 1/5 OF ALL VOLUNTEER MENTIONS FROM THE 4 PERCENT OF VOLUNTEERS WITH MEGAPHONES!
WHAT THE DATA SHOWS Large chunks of the urban population, and even of many rural populations, are accessible through mass media approaches. However, we are unlikely to achieve herd immunity in campaigns without house to house mobilization. In addition to campaigns, intercampaign house canvassing, 1 ½ years after the SIA, is a promising possibility to reduce the risk of outbreaks between campaigns.
METHODS FOR EVALUATING COMPARATIVE PERFORMANCE OF H2H AND CONVENTIONAL APPROACHES
WHY WE NEED MORE SPOT SURVEYS Cluster coverage surveys, with more scientific rigor, are not always done, and rarely permit comparison between areas with and without house visiting. Admin coverage data are based on high side population figures (Eritrea) or low side population figures (Uganda). >>100% coverage = high degree of flakiness; true of ½ of all districts in Uganda’s 2012 measles SIA. Data retention by health workers (Senegal, Kampala) makes it impossible to calculate SIA admin coverage.
COSTING OF HOUSE TO HOUSE MOBILIZATION Vitamin m, the indispensable micronutrient Single partner funding by American Red Cross is not a viable option for H2H mobilization to go to scale.
ADDED COST PER BENEFICIARY, H2H STRATEGY, FIVE MOST RECENT NATIONAL CAMPAIGNS, AVERAGE $0.32. UNIT COSTS VARY. TANZANIA FINANCED DAR ES SALAAM, WITH LOW UNIT COSTS. NAMIBIA FINANCED RURAL AREAS.
CONCLUSIONS • In areas with H2H mobilization, measles SIA cost per child rises from ~$1 to ~$1.32 or more. • We need to be selective in choosing areas for H2H. • Selection criteria used by American Red Cross and, in some countries, UNICEF: • Underserved populations, especially slums • Areas with low coverage and/or high cases based on case based surveillance • Geographically remote areas
CONCLUSIONS (CONT.) Some countries (Kenya, Burkina Faso) have widespread viral seeding from town to country. There, it may be necessary there to target whole cities, not just slums. In some settings, the dollar goes farther in urban H2H mobilization (Tanzania vs. Namibia). Where funding is short, first priority goes to underserved urban and periurban areas.
THE MAGIC FORMULA There is no magic formula for targeting areas to cover through H2H. Where viral seeding is well documented, target the source of the viral seeding. Where coverage data are reliable, target areas with low coverage. Where case based surveillance is good, target areas with cases (Burundi: 4/17 regions were home to 29/30 confirmed measles cases).
URBAN PARTICULARITIES Weekend SIA start is preferable; no traffic jams to tie up logistics; pulpit announcements on Fridays and Sundays Multilingual house visitors and vaccinators are needed – Dakar, Nairobi, for example. Mapping of neighborhoods with many migrants and floating populations, for special emphasis by gov’t, RC and other partners
H2H CANVASSING FOR ROUTINE IMMUNIZATION? American Red Cross & partners need to consult on how best to apply lessons learned from SIAs to routine immunization. A network of volunteers already exists to sensitize the community. Possible modalities: birth registration and follow-up; periodic village canvasses; linkages to health facilities for defaulter follow-up
SO WHERE IS H2H GOING? Depends on decisions made by the MRI, as by the GPEI in 2001, when the polio initiative opted for H2H OPV SIAs. If H2H mobilization goes global with measles, as with polio, then more resources and partners will be needed. You can’t go global on a shoestring, and you can’t do it with 1 or 2 partners, as at present. Decision whether to go global with H2H should predate any WHA resolution. No 1988-2001 gap as with GPEI, SVP!
THANK YOU/ASANTE SANA/ AMESEGNALEHU/SIYABONGA/ MERCI/OBRIGADO/MUCHAS GRACIAS AMESEGNALEHU ANSAKUSU ARIGATO ASANTE SANA BAIE DANKIE BARKA BEDANKT BINOBONDI DEUS PAGARAPUSUNKI DHANJABHAT DJERE DIEUF DIOKO NDIAL DYARAAMA/FOOFU DZIĘKUJEMY DUNABAT EFHARISTO ESE GELETOMA GRAMACI (PROVENÇAL) HAKHENTSA HARTELIJK DANK! HSEHSE HVALA INITCHIE INKOSI KAMSAHAMNIDA KANIMAMBO KEAITUMETSE KEA LEBOHA KHOBKHUN MAG KIITOS PALION (FINNISH) KÖSZÖNÖN LONGONIA MINGI LOSAKA MADLOBT (DIDI MADLOVA) MAHADSANIT MANAM MAZVITA MEDASE MERCI MILLE GRAZIE MIRISE MISAOTRA MUCHAS GRACIAS MURAKOZE CYANE MWASHUMA MPUSIYA NAGODE NAMVERA NAPANDULA NASOM NATONDI NDAU YA NDUNA NDA BOKA NDIYABULELA NGASSAKIDILA • OKUHEPA • PANDU • RE A LEBOGA • RO LIVHUWA • SALAMAT • SHNORHAKALOUTYOUN • SINGUILA MINGUI • SHUKRAN • SIYABONGA • SOSONGO • SPASIBA • TATENDA • TERIMAKASIH • TEŞEKKŰRLER • TODAH RABAH • TSE ZU TIN BA DEH • TVASAKIOILA • TWATASHA • TWATOTELA • VIELEN DANK • VILLMOLS MERCI • WAKOOZECHANE • WEBAALE NNYO • YABONGA • YAQENYILEY • ZIKOMO