Download
1 / 25
270 likes | 476 Views
Shape 2012 November 2, 2012. Lessons learned from the Heinz Nixdorf Recall study. Raimund Erbel for the Ivestigator Group of the Heinz Nixdorf Recall study Department of Cardiology West-German Heart Center University Duisburg-Essen

E N D
Shape 2012 November 2, 2012 Lessons learned from the Heinz Nixdorf Recall study Raimund Erbel for the Ivestigator Group of the Heinz Nixdorf Recall study Department of Cardiology West-German Heart Center University Duisburg-Essen www.recall-studie.uni-essen.de erbel@uk-essen.de
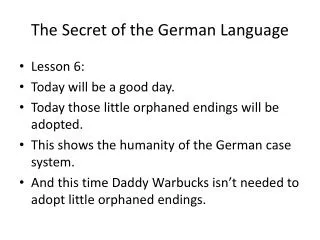
Improvement of Risk Prediction for Coronary Events using Signs of Subclinical Atherosclerosis and Biomarkers Proportion of in-Hospital CHD Death Proportion of CHD deaths (%) within 28 days occurring in hospital by sex, age, and calendar year, 1991 to 2006. Women Men 1992 2000 2006 1992 2000 2006 Kerstin Dudas et. al. Circulation 123:46-52, /2011 Leszek K Borysiewicz
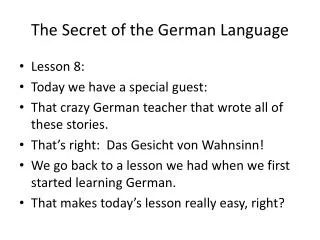
Improvement of Risk Prediction for Coronary Events using Signs of Subclinical Atherosclerosis and Biomarkers Most Deaths of AMI occur out of the hospital Mortality due to CHD in the hospital (within 28 days) and out of the hospital per 100 000 population 35 10 84 years of age, 1991 to 2006. Kerstin Dudas et. al. Circulation 123:46-52, /2011
Assmann et al. Circulation 105:310-315, 2002 JAMA 385, 2001 • Step: Score based Risk – Stratification A. Framingham B. PROCAM Graham I et al EJCPR 14 (suppl 2:S1-113), 2007
advice for healthy lifestyle intensive therapy / risk factor modification 2. Step based Risk – Categorization < 10% / 10 years Low risk - Intermediate risk detection of signs of subclinical atherosclerosis 10 – 20% / 10 years + High risk = equivalent to post AMI > 20% / 10 years • Greenland et al. Circulation 2000;101:111-116 Greenland et al. Circulation 2001;104:1863-1867 • NCEP / ATP III JAMA 2001;285:2486-97 # Erbel et al. Atherosclerosis 2007;197:662-72
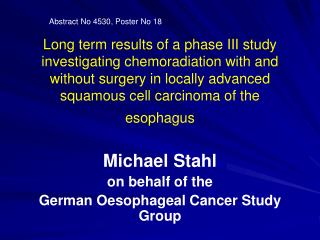
2. Step: Risk Prediction for Coronary Events using Framingham Risk Score in HNR study 37 / 1303 2.46 (1.49-4.07) 29 / 498 5.04 (2.98-8.53) 25 / 2165 1.0 Events / # atRisk: Relative Risk: p=0.003 p=0.0003 Observed 5-yr Event Rate [%] 5.8 % 2.8 % 1.2 % Framingham Risk Score Erbel R et. al. JACC 56:1397-406, 2010
for healthy lifestyle intensive therapy / risk factor modification 3. Step: subclinical signs of atherosclerosis used for further risk stratification Prevalence of risk categories in Germany Men / Women - < 10% / 10 years Low Risk 30% / 71% • Imaging techniques • Non imaging techniques • Stress ECG (M 45 - 60 J) • Biomarker Intermediate Risk 10 – 20% / 10 years 39% / 20% > 20% / 10 years High Risk 31% / 9% + Data from the Heinz Nixdorf Recall Study# (incl. ATP III risk equivalents*) • Greenland et al. Circulation 2000;101:111-116 Greenland et al. Circulation 2001;104:1863-1867 • NCEP / ATP III JAMA 2001;285:2486-97 # Erbel et al. Atherosclerosis 2007;197:662-72
Imaging of Coronary Subclinical Atherosclerosis EKG ECHOCARDIOGRAPHY Non invasive Methods SCINTIGRAPHY PET MRT CT/CTA Vasomotion testing OCT IVUS/ICD IRS Invasive Methods CORONARY ANGIOGRAPHY 0% 20% 45% 50% 70% 90% Remodeling Life time Di000802 modified according to Erbel R et al HERZ 32:351-55, 2007 originally ERBEL R HERZ 21: 75-77, 1996
Non-Invasive Imaging of Subclinical Coronary Atherosclerosis using Computed Tomography Score 49 No CAC RVOT LAD Ao CAC 56 year M LM 51 year M Score 115 Score 2609 64 year F 50 year M Detection - Distribution – Quantification
Non-Invasive Imaging of Subclinical Coronary Atherosclerosis using Computed Tomography - < 20 s scan time - 1-1.3 mSv X-ray exposure - 100 ms acquisition time - standardized protocols: Agatston-Score - 15-20 min total time - 0.94 Kappa value for inter- institutional variation Imaging of coronary artery calcification as a specific sign of atherosclerosis Agatston et al. JACC 15:827-32, 1990 Hunold P et al Radiology 226:14552,2003 Schmermund et al . Z Kardiol 92:I/385,2003
3. Step: Improving Risk Prediction for Coronary Events using Signs of Coronary Subclinical Atherosclerosis by CT Events / # atRisk: Crude Relative Risk: FRS-adjusted* RR: 11 / 1287 1.0 1.0 24 / 1624 1.73 (0.85-3.52) 1.46 (0.71-3.00) 23 / 659 4.08 (2.00-8.33) 3.06 (1.48-6.32) 33 / 396 9.75 (4.97-19.11) 6.25 (3.01-13.00) p=0.0007 p=0.002 p=0.13 Observed 5-yr Event Rate [%] 8.3 % 3.5 % 1.5 % 0.9 % CAC Scoring Erbel R et. al. JACC 56:1397-406, 2010
Improvement of Risk Prediction for Coronary Events using Signs of Coronary Subclinical Atherosclerosis by CT categories Meta-analysis HNR study Meta-analysis HNR study Meta-analysis HNR study Meta-analysis HNR study Greenland et al. ACCF/AHA 2007 Clinical expert consensus document JACC 115:402, 2007 Erbel et al JACC 56:1397-406, 2010
Improvement of Risk Prediction for Coronary Events using Signs of Coronary Subclinical Atherosclerosis by CT Rotterdam Study Elias-Smale SE et al JACC 56:1407-14, 2010
Improvement of Risk Prediction for Coronary Events using Signs of Subclinical Atherosclerosis by CT demonstrated by the Net Reclassification Improvement NRI NRI: 20.8% (p=0.0004) low intermediate high Erbel R et. al. JACC 56:1397-406, 2010
Improvement of Risk Prediction for Coronary Events using Signs of Subclinical Atherosclerosis by CT demonstrated by the Net Reclassification Improvement NRI NRI: 20.8% (p=0.0004) Erbel R et. al. JACC 56:1397-406, 2010
Improvement of Risk Prediction for Coronary Events using Signs of Subclinical Atherosclerosis by CT demonstrated by the Net Reclassification Improvement NRI Comparison to the FRS 6-20% instead of 10-20% NRI = 30.6% (p<0.0001) Erbel R et. al. JACC 56:1397-406, 2010
advice for for healthy lifestyle intensive therapy / risk factor modification 3. Step: Improving Risk Prediction for Coronary Events using Signs of Inflammation – a Biomarker Prevalence of risk categories in Germany Men / Women - < 10% / 10 years Low Risk 30% / 71% Detection of signs of risk for CV events Biomarker Intermediate Risk 10 – 20% / 10 years 39% / 20% > 20% / 10 years High Risk 31% / 9% + Data from the Heinz Nixdorf Recall Study# (incl. ATP III risk equivalents*) • Greenland et al. Circulation 2000;101:111-116 Greenland et al. Circulation 2001;104:1863-1867 • NCEP / ATP III JAMA 2001;285:2486-97 # Erbel et al. Atherosclerosis 2007;197:662-72
Lipoprotein (a) Univariate Analysis forcardiac deah, AMI, revascularisation Homocystein Cholesterol (TC) n = 28.263 * n = 4.348 LDL - Cholesterol (LDLC) TC/HDLC - Ratio HS - CRP * Calcium Score 0 0.5 1 2 3 4 5 6 7 8 9 10 11 Relative Risk of Future Cardiovascular Events Improvement of Risk Prediction for Coronary Events using Biomarkers Ridker PM et al Circulation 103: 1813, 2001 *O‘Malley PG et al Am J Cardiol 85: 945, 2001
3. Step: Improving Risk Prediction for Coronary Events using the Biomarker – hs-CRP Events / # atRisk: Crude Relative Risk: FRS-adjusted* RR: 23 / 1387 1.0 1.0 31 / 1682 1.11 (0.65-1.90)0.93 (0.54-1.60) 37 / 897 2.49 (1.49-4.16) 1.87 (1.09-3.21) p=0.0006 Observed 5-yr Event Rate [%] p=0.70 4.1 % 1.8 % 1.7 % hsCRP Categories Möhlenkamp S et al JACC 2011 in press
Improvement of Risk Prediction for Coronary Events using the Biomarker – hs-CRP vs CAC mg/L hs-CRP Möhlenkamp S et al J Am Coll Cardiol. 2011 ;57:1455-64
Improvement of Risk Prediction for Coronary Events using the Biomarker – hs-CRP vs CAC 1 0.75 AuROC-Curve: FRS only: 0.691 (0.638-0.744) p=0.19 p=0.34 Sensitivity 0.5 FRS+hsCRP: 0.704 (0.652-0.757) p=0.0074 FRS+log2(CAC+1): p=0.014 0.752 (0.700-0.804) 0.25 FRS+hsCRP+log2(CAC+1): 0.760 (0.710-0.810) 0 0 0.25 0.5 0.75 1 1-Specificity Möhlenkamp S et al J Am Coll Cardiol. 2011 ;57:1455-64
Improvement of Risk Prediction for Coronary Events using the Biomarker – hs-CRP Net Reclassification Improvement NRI: 7.8% (p=0.14) Möhlenkamp S et al J Am Coll Cardiol. 2011 ;57:1455-64
Improvement of Risk Prediction for Coronary Events using Signs of Subclinical Atherosclerosis and Biomarkers Risk Marker / Factor: NRI p-value Reference Multiple Biomarker Score 26.7% p=0.005 (Zethelius, NEJM 2008)* (Troponin I, NT-proBNP, Cystatin C, CRP) Multiple Biomarker Score 14.6% p=NS (Melander, JAMA 2009)* (MR-proADM, NT-proBNP) HDL-Cholesterol (Framingham) 12.1% p<0.001 (Pencina, Stat Med 2008) HDL-Cholesterol (SCORE-Data) 2.2% p=0.006 (Cooney, EJCPR 2009) hsCRP (women) 5.7% p<0.0001 (Cook, Ann Int Med 2006) hsCRP (men and women) 11.8% p<0.009 (Wilson Cirulation 2008) hsCRP (men) 14.1% p<0.001 (Ridker, Circulation 2008)* HbA1c (men) 3.4% p=0.06 (Simmons, Arch Int Med 2008) HbA1c (women) - 2.2% p=0.27 (Simmons, Arch Int Med 2008) CAC HNR(ATP III, FRS 10-20%, 6-10%) 18.8, 21.7%, 30.6% p=0.0002 (Erbel, JACC 2010)* Rotterdam FRS 10 – 20 % 14% p<0.01 also hard events,older MESA FRS 6 – 20% 30% p<0.001 also soft endpoints modified from Cooney et al. JACC 54 :1209-1227, 2009 Erbel R et al JACC 56 :1397- 406, 2010
Improvement of Risk Prediction for Coronary Events using Signs of Subclinical Atherosclerosis and Biomarkers Risk Marker / Factor: NRI p-value Reference Multiple Biomarker Score 26.7% p=0.005 (Zethelius, NEJM 2008)* (Troponin I, NT-proBNP, Cystatin C, CRP) Multiple Biomarker Score 14.6% p=NS (Melander, JAMA 2009)* (MR-proADM, NT-proBNP) HDL-Cholesterol (Framingham) 12.1% p<0.001 (Pencina, Stat Med 2008) HDL-Cholesterol (SCORE-Data) 2.2% p=0.006 (Cooney, EJCPR 2009) Heart Rate 1.1% p=NS (Cooney, ESC 2009, Abstract) hsCRP (women) 5.7% p<0.0001 (Cook, Ann Int Med 2006) hsCRP (men and women) 11.8% p<0.009 (Wilson Cirulation 2008) hsCRP (men) 14.1% p<0.001 (Ridker, Circulation 2008)* hsCRP (total 7.8% p <0.14 (Möhlenkamp JACC 2011) HbA1c (men) 3.4% p=0.06 (Simmons, Arch Int Med 2008) HbA1c (women) - 2.2% p=0.27 (Simmons, Arch Int Med 2008) CAC (ATP III, FRS 10-20%, 6-10%) 18.8, 21.7%, 30.6% p=0.0002 (Erbel JACC 2010)* modified from Cooney et al. JACC 54 :1209-1227, 2009 Erbel R et al JACC 56 :1397- 406, 2010
Improvement of Risk Prediction for Coronary Events using Signs of Subclinical Atherosclerosis and Biomarkers Conclusion In comparison to other signs of subclincial atherosclerosis CAC seems to be the method of choice for improvement of risk prediction. And cardiology has to turn its attention to prevention, because here the biggest target for risk improvement has to be recognized as the majority of patient (60 to 80 %), who die from AMI, die outside the hospital and do not reach the hospital.