Download
1 / 47
711 likes | 1.43k Views
Acute Rheumatic Fever Dr. Toba kazemi, MD 2752-2757 Harrison 2012 31.02.1391. Objectives. Etiology Epidemiology Pathogenesis Pathologic lesions Clinical manifestations & Laboratory findings Diagnosis & Differential diagnosis Treatment Prevention Prognosis. Introduction. Introduction.

E N D
Acute Rheumatic FeverDr. Toba kazemi, MD2752-2757Harrison 201231.02.1391
Objectives • Etiology • Epidemiology • Pathogenesis • Pathologic lesions • Clinical manifestations & Laboratory findings • Diagnosis & Differential diagnosis • Treatment • Prevention • Prognosis
Introduction Introduction • Acute rheumatic fever (ARF) is a multisystem disease resulting from an autoimmune reaction to infection with group A streptococcus.(GAS) • Although many parts of the body may be affected, almost all of the manifestations resolvecompletely. • The exception is cardiac valvular damage [rheumatic heart disease (RHD)], which may persist after the other features have disappeared
Introduction Introduction • ARF and RHD are diseases of poverty • They were common in all countries until the early 12th century, when to decline in industrialized nations • This decline was largely attributable to : • improved living conditions : less crowded housing ,better hygiene- reduced transmission of GAS • The introduction of antibiotics and improved systems of medical care
Introduction • RHD is the most common cause of heart disease in children in developing countries and is a major cause of mortality and morbidity in adults as well • Some 95% of ARF cases and RHD deaths now occur in developing countries. • These "hot spots" are sub-Saharan Africa, Pacific nations, Australasia, and the Indian subcontinent
Epidemiology • Initial episode : aged 5-14 years. • rare in persons aged >30 years. • Recurrent episodes of ARF remain relatively common in adolescents and young adults. • Prevalence RHD: Peaks between 25 - 40 years. • M:F equally except Sydenham’s chorea which is more common in girls • RHD more commonly affects females ,F/M=2
Pathogenesis • ORGANISM FACTORS: • infection of the upper respiratory tract (pharyngitis)withgroup A streptococci. • it is now thought that any strain of group A streptococcus has the potential to cause ARF. • Potential role of skin infection and of groups C and G streptococci are currently being investigated. • Different serotypes from strains causing impetigo or glomerulonephritis • HOST FACTORS
Diagrammatic structure of the group A beta hemolytic streptococcus Antigen of outer protein cell wall of GABHS induces antibody response in victim which result in autoimmune damage to heart valves, sub cutaneous tissue,tendons, joints & basal ganglia of brain Capsule Cell wall Proteinantigens Group carbohydrate Peptidoglycan Cyto.membrane Cytoplasm …………………………………………………...
Pathogenesis • HOST FACTORS • 3-6% of any population may be susceptible to ARF, • an inherited characteristic: • Findings of familial clustering of cases and concordance in monozygotic twins-particularly for chorea-confirm. • Particular (HLA) class II • High levels of circulating mannose-binding lectin and polymorphisms of transforming growth factor ~l gene and immunoglobulin genes. • High-level expression of analloantigen present on B cells,D8-17,
summary Cause of “Acquired” heart disease in children. ( “world-wide” but not in USA ) - AHA: >3200 deaths in US, related to RF/RHD in 2004. Sequelae of inadequately “treated” strep. pharyngitis. ( “strep throat” ) “Highly” Uncommon - < 1% of untreated infections. - Gp A beta-hemolytic - rheumatogenic strains – “M” proteins. - 1/3rd of cases follow “inapparent” strep infections. A “Non-Suppurative” Systemic Inflammatory illness occuring 1 - 2 wks following a Strep.Infection. Pathogenesis - “Autoimmune” mediated. Multiple systems affected. (Joints, Skin, CNS & Heart !) Primarily affects: 3 –15 year old age group.
Pathologic Lesions • Fibrinoid degeneration of connective tissue,inflammatory edema, inflammatory cell infiltration & proliferation of specific cells resulting in formation of Ashcoff nodules, resulting in- • Pancarditis in the heart • Arthritis in the joints • Ashcoff nodulesinthe subcutaneous tissue • Basal gangliar lesions= chorea
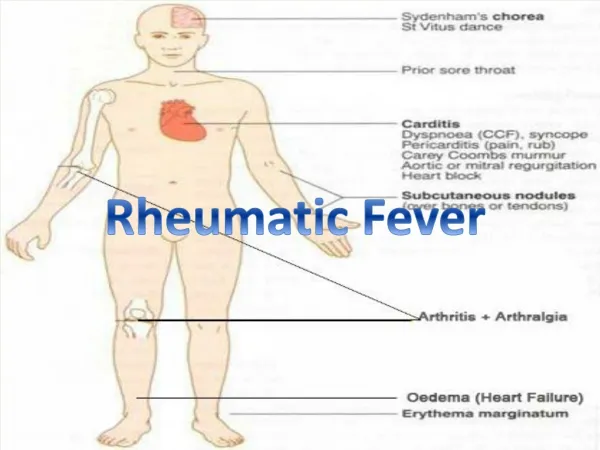
CLINICAL FEATURES • The most common clinical presentation of ARF: • polyarthritis ,fever • Polyarthritis :60-75% of cases • carditis : 50-60% • chorea :<2% to 30%. • Erythema marginatum: rare, <5% • subcutaneous nodules : rare, <5%
CLINICAL FEATURES • There is a latent period of -3 weeks (1-5 weeks) • The exceptions : • chorea • indolent carditis, • many patients report a perior sore throat • commonly subclinical
1.Arthritis • objective evidence of inflammation, hot,swollen,red and/or tender joints. • Polyarthritis; more than one joint • Migratory; moving from one joint to another over a period of hours. • affects the large joints-most commonly the knees, ankles, hips, and elbows- • asymmetric. • in 80%,involved joints are exquisitely tender • The pain is severe and usually disabling until anti-inflammatory medication is commenced
1.Arthritis-continued • Less severe joint involvement is also relatively common but qualifies only as a minor anifestation. • Arthralgia without objective joint inflammation usually affects large joints in the same migratory pattern as polyarthritis. • In some populations, aseptic monoarthritis may be a presenting feature of ARF. • This may occur because of early commencement of antiinflammatory medication before the typical migratory pattern is established Without Complication.
1.Arthritis-continued • highly responsive to salicylates and other (NSAIDs). • joint involvement that persists more than 1 or 2 days after starting salicylates is unlikely to be due to ARF. • Conversely, if salicylates are commenced early in the illness, before fever and migratory polyarthritis have become manifest, it may be difficult to make a diagnosis of ARF. • salicylates and other NSAIDs should be withheld-and pain managed with acetaminophen or codeine-until the diagnosis is confirmed
2.Carditis • Manifest as • Pancarditis (endocarditis, myocarditis ,pericarditis), • in 40-50% of cases • the only manifestation of ARF that leaves a sequelae & permanent damage to the organ • Up to 60% of patients with ARF progress to RHD • mitral valve(MV) is almost always affected. • sometimes together with the aortic valve(MV+AV) • isolated aortic valve involvement is rare.
2.Carditis-continued • Early valvular damage leads to regurgitation • Valvulitis occur in acute phase(MR,AR) • Chronic phase- usually as a result of recurrent episodes, leaflet thickening, scarring, calcification, and valvular stenosis may develop (MS,MR,AS,AR)=multivalvular • Myocardial inflammation may affect electrical conduction pathways, leading to P-R interval prolongation (firstdegree AV block or rarely higher-level block) and softening of the first heart sound. • Pericardial effusion • CHF
Mainly in girls of 1-15 yrs age occurs in the absence of other manifestations, follows a prolonged latent period after GAS May appear even 6/12 mo after ARF attack choreiform movements affect head (causing darting movements of the tongue) and the upper limbs may be generalized or restricted to one side of the body (hemi-chorea). Clinically manifest as-clumsiness, deterioration of handwriting,emotional lability or grimacing of face Clinical signs- pronator sign, jack in the box sign , milking sign of hands 3.Sydenham Chorea
3.Sydenham Chorea • The chorea varies in severity • In mild cases it may be evident only on careful examination, while in the most severe cases the affected individuals are unable to perform activities of daily living and are at risk of injuring themselves. • Chorea eventually resolvescompletely, usually within 6 weeks.
4.Erythema Marginatum • Occur in <5%. • The classic rash of ARF is erythema marginatum • pink macules that clear centrally, leaving a spreading edge Pale center with red irregular margin • The rash is evanescent, appearing and disappearing before the examiner's eyes. • It occurs usually on the trunk, sometimes on the limbs, but almost never on the face. • Worsens with application of heat • They are a delayed manifestation, appearing 2-3 weeks after the onset of disease, last for just a few days up to 3 weeks, and are commonly associated with carditis
5.Subcutaneous nodules • painless, small (0.5-2 ern), mobilelumps beneath the skin overlying bony prominences, • particularly of the hands, feet, elbows, occiput, and occasionally the vertebrae. • delayed manifestation, • appearing 2-3 weeks after the onset of disease, • last for just a few days up to 3 weeks, • commonly associated with carditis
Other features (Minor features) • Fever-occurs in most cases of ARF, rarely in cases of pure chorea. • Although high-grade fever (39°C) is the rule,lower grade temperature elevations are not uncommon. • Arthralgia,Pallor,Anorexia,Loss of weight • Elevated acute-phase reactants are also present in most cases. • CRP and ESR are often dramatically elevated. • Occasionally the peripheral leukocyte count is mildly elevated
Clinical Features:summary Polyarthritis– w/ low grade fever, large joints, ( > 75%) migratory , with no permanent dysfunction. Carditis -pancarditis( pericarditis, cardiomegaly, or valvulitis) ( ~ 50%) (valvulitis is the most serious manifestation.) Chorea – late occurrence, 3 - 4 months after ( ~ 10%) infection, self-limiting, resolves in 1- 3 months. Erythema Marginatum – “classic” truncal rash, ( ~ 10%) migratory - appears & disappears within hours. (pink rash – irregular red edges – clear center) Subcutaneous Nodules – late occurs late (1 - 2%) ( months after infection), painless small nodules over bony prominences - elbows, knees, spine.
Laboratory Findings • high ESR,CRP,WBC • EVIDENCE OF A GAS infection: • With the exception of chorea and low-grade carditis, preceding GAS infection is essential in making the diagnosis of ARF. • throat swab culture or rapid antigen test ;As most cases do not have a positive, serologic evidence is usually needed. • The most common serologic tests are the antistreptolysin0 (ASO) and anti-DNase B (ADB) titers. .
Laboratory Findings • ECG- prolonged PR interval, 2nd or 3rd degree blocks,ST depression, T inversion • Chest X-ray;cardiomegaly • 2D Echo cardiography- valve edema,mitral regurgitation, LA & LV dilatation,pericardial effusion,decreased contractility
OTHERPOST-STREPTOCOCCAL SYNDROMES • 1-Post-streptococcal reactive arthritis (PSRA): • small-joint involvement ,often symmetric • a short latent period following streptococcal infection (usually <1 week) • causation : nongroup A -hemolytic streptococcal infection • slower responsiveness to salicylates • the absence of other features of ARF, particularly carditis.
OTHER POST-STREPTOCOCCAL SYNDROMES • 2- Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS) • tic disorders and obsessive-compulsive symptoms with GAS. • PANDAS are not to be at risk of carditis, unlike patients with Sydenham's chorea. • The diagnoses of PANDAS and PSRA should rarely be made in populations with a high incidence of ARF.
Diagnosis • Rheumatic fever is mainly a clinical diagnosis • No single diagnostic sign or specific laboratory test available for diagnosis • Diagnosis based on MODIFIED JONES CRITERIA • Jones Criteria – Diagnosis of ARF requires 2 major criteria OR one major and two minor criteria evidence of recent streptococcal infection
2002-2003 WHO Criteria for the Diagnosis of ARF and RHD (Based on the 1992 Revised Jones Criteria
Jones Criteria* Major Minor Polyarthritis Arthralgia Carditis Prolonged PR Chorea Elevated CRP, ESR Erythema marginatum Fever Subcutaneous Nodules Elevated WBC evidence of a prior strep. infection ( increaser ASO or anti-DNAse AB) or Hx of (+) C/S or Rapid Strep Test
Exceptions to Jones Criteria • Chorea alone, if other causes have been excluded • Insidious or late-onset carditis with no other explanation • Patients with documented RHD or prior rheumatic fever,one major criterion,or of fever,arthralgia or high CRP suggests recurrence
Treatment • Step I- primary prevention (eradication of streptococci) • Step II- anti inflammatory treatment (aspirin,steroids) • Step III- supportive management & management of complications • Step IV- secondary prevention (prevention of recurrent attacks)
Treatment • Primary prophylaxis • the timely and complete treatment of group A streptococcal sore throat with antibiotics . • If commenced within 9 days of sore throat onset, a course of penicillin (as outlined above for treatment of ARF) will prevent almost all cases of ARF that would otherwise have developed. • Treatment of choice is still Penicillin • Oral: penicillin, 500 mg BID (250 mg for children <27 kg) PO, amoxicillin 50 mglkg (max 1 g) daily • Parenteral: a single dose of 1.2 million units (600,000 units for children < 27 kg) 1M benzathine penicillin G. • Treatment administered within 10 days of onset of illness has been shown to prevent ARF.
Treatment • anti inflammatory treatment • used for the treatment of arthritis, arthralgia, and fever, once the diagnosis is confirmed. • They are of no proven value in the treatment of carditis or chorea. • Aspirin is the drug of choice. • An initial dose of 80-100 mg/kg per day in children (4-8 g/d in adults) in 4-5 divided doses is often needed for the first few days up to 2 weeks • When the acute symptoms are substantially resolved, the dose can be reduced to 60-70 mg/kg per day for a further 2-4 weeks.
Treatment • SECONDARY PREVENTION • patients with ARF are dramatically higher risk than the general population of developing a further episode of ARF after GAS. • they should receive long-term penicillin prophylaxis to prevent recurrences. • The best antibiotic is benzathine penicillin G (1.2 million units, or 600,000 units if ≤27 kg) every 4 weeks. • It can be given every 3 weeks, or even every 2 weeks, to persons considered to be at particularly high risk • Oral penicillin V (250 mg) BID • oral penicillin is less effective than benzathine penicillin G. • Penicillin allergic patients can receive erythromycin 250 mg BID
Antibiotics “NOT” Recommended for Strep. Pharyngitis: Sulfonamides Trimethoprim / Sulfamethoxazole Fluoroquinolones Tetracyclines / Doxycycline / Minocycline