Download
1 / 26
510 likes | 3.07k Views
Anesthesia with Cardiac Tamponade. By R3 黃信豪. Brief history (1). A 1 y/o female patient, about 10.9 kg. Congenital VSD was diagnosed at birth. VSD repair was performed in 93-07-26 in NTUH. No residual VSD was noted in f/u TTE report. Brief history (2).

E N D
Anesthesia with Cardiac Tamponade By R3黃信豪
Brief history (1) • A 1 y/o female patient, about 10.9 kg. • Congenital VSD was diagnosed at birth. • VSD repair was performed in 93-07-26 in NTUH. • No residual VSD was noted in f/u TTE report.
Brief history (2) • Poor appetite and daily activity decreased were noted for 3 days. • Patient was sent to 金門縣立醫院, and pericardial effusion was told. So patient was transferred to our hospital in 93-08-11. • Patient was admitted at 4C2 ICU, and TTE was performed immediately. Pericardial effusion was confirmed, so emergent operation for effusion drainage was arranged.
Brief history (3) • Patient was sent to OR with A-line inserted and a 24G peripheral line. • HR was about 135-150 per min. BP was around 100/60 mmHg without any inotropic agent, and would be dropped to 85/50 mmHg when she calmed down. SpO2 was about 98-100. • No cyanosis or jugular vein engorged was noted since patient came to the hospital.
Brief history (4) • After CVS doctors arrived, induction was performed. medication: Ketamine 25 mg Atropine 0.1mg Nimbex 3 mg intubation: with 5.0 ET tube fixed 13 cm checked by stethoscope • After intubation, ventilator was used.
Brief history (5) • The HR was kept around 120-140 per min. The BP was around 90/60 mmHg. SpO2 was still about 100. • pericardiotomy via subxiphoid approached for effusion drainage was performed immediately. About 50 ml clear and yellowish fluid was drainage. Then BP was elevated to 120/ 70 mmHg after the procedure. • After replacing a chest tube in pericardial space for drainage, the wound was closed. Then patient was sent to 4A2 ICU for further care.
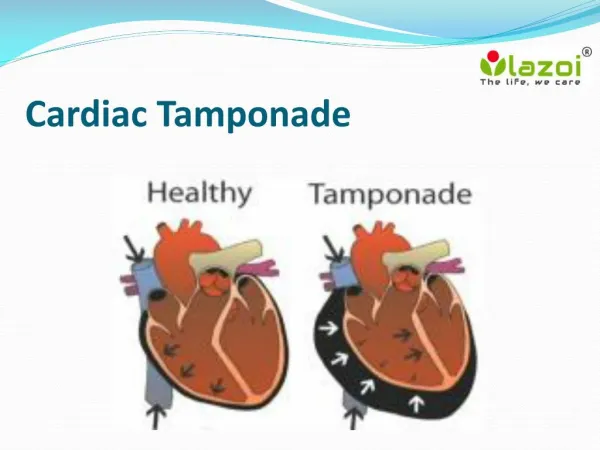
Cardiac tamponade: the accumulation of fluid in the pericardium in an amount sufficient to cause serious obstruction to the inflow of blood to ventricle results in cardiac tamponade. The three principal features of tamponade are: 1.elevation of intracardiac pressures 2.limitation of ventricular fillng 3.reduction of cardiac output Definition
The pericardium, which is the membrane surrounding the heart, is composed of 2 layers. The parietal pericardium is the outer fibrous layer; the visceral pericardium is the inner serous layer. The pericardial space normally contains 20-50 mL of fluid
The most common causes are: • neoplastic disease • idiopathic pericarditis • uremia • the following cardiac operation • trauma: • The amount of fluid necessary to produce the critical state: Acute tamponade: 150-200 ml Chronic tamponade: 1000-2000 ml
The three phase of hemodynamic changes in cardiac tamponade: (by Reddy et. al.) • Phase I: The accumulation of pericardial fluid causes increased stiffness of the ventricle, requiring a higher filling pressure. During this phase, the left and right ventricular filling pressures are higher than the intrapericardial pressure. • Phase II: With further fluid accumulation, the pericardial pressure increases above the ventricular filling pressure, resulting in reduced cardiac output. • Phase III: A further decrease in cardiac output occurs, which is due to equilibration of pericardial and left ventricular (LV) filling pressures.
The features of the cardiac tamponade (1) A.clinical features • Shortness of breath • Weakness and fatigue • Anxiety • tachycardia • Jugular vein engorged—Beck triad • Cyanosis
The features of the cardiac tamponade (2) • Beck triad: • increased jugular venous pressure • hypotension, • diminished heart sounds • Pulsus paradoxus: A greater than normal (10 mmHg) inspiratiory decline in systolic arterial pressure. • Kussmaul’s sign :paradoxical increasing venous pressure during inspiratory • Ewart’s sign :area of dullness, with bronchial breath sounds and bronchophony below the angle of the left scapula
The features of the cardiac tamponade (3) • The ECG of cardiac tamponade: 1.Low electrical voltage 2.P-R segment depression • ECG signs that are suggestive, but not diagnostic, of pericardial effusion and cardiac tamponade. Because these ECG findings cannot reliably identify these conditions, we conclude that 12-lead ECG is poorly diagnostic of pericardial effusion and cardiac tamponade ~~ by Mark J. Eisenberg, MD
The features of the cardiac tamponade (4) • The CXR of cardiac tamponade: The x-ray may show an enlarged cardiac “silhouette” due to an excessive volume of pericardial fluid, especially when more than 200 milliliters of fluid has built up in the pericardium.
The features of the cardiac tamponade (5) • The echocardiogram of cardiac tamponade: • echo free space between epicardium and pericardium • heart Swinging
The treatment of cardiac tamponade (1) • Medical care: a.oxygen b.volume expansion c.bed rest with lower limbs elevation d.inotropic agents use~dobutamine
The treatment of cardiac tamponade (2) • Invasive procedure: a. Pericardiocentesis b. Subxiphoid percutaneous drainage c. Percutaneous balloon pericardiotomy d. Surgical creation of a pericardial window e. Pericardio-peritoneal shunt f. Pericardiodesis or sclerosing the pericardium g. Pericardiectomy
About the anesthesia plan in cardiac tamponade. • The plan should • include monitoring of the important hemodynamic variables. • omit drugs and minimize manipulations that decrease venous return, reduce heart rate, produce hypotension, result in hypoxemia, or impair ventricular contractility
The monitors needed for cardiac tamponade • SpO2 • A-line • ECG –not for diagnosis, for arrhythmia detection • CVP • Swan-Ganz catheterization
The route for induction • Inhalation induction: All modern volatile anesthetics, including desflurane and sevoflurane, depress contractile function in normal myocardium in vitro and in vivo----Not suitable for the case of cardiac tamponade!!!! • Intravenous induction: etomidate or ketamine
Left Ventricular Stroke Work Index(LVSWI) = SV/BSA * (MAP-PAWP) * 0.0136
By “Hemodynamic response to ketamine and diazepam in dogs with acute cardiac tamponade” • Ketamine, 2 mg/kg intravenously resulted in an improvement of cardiac output from 1.2 +/- 0.5 L/min to 2.2 +/- 0.3 L/min (p less than 0.05 ) • Five dogs with intrapericardial pressure above 10 mmHg did not respond to ketamine. • Emergency subxiphoid percutaneous drainage: This is a life-saving bedside procedure.
The mode of ventilation • Positive pressure ventilation positive pressure ventilation will further embarrasses venous return and cardiac output – contraindication !!! • Spontaneous ventilation the best choice of cardiac tamponade until the tamponade is relieved.
The inotropes and chronotropes • Epinephrine - b21 2 mg/min • b1 + b2 2–10 mg/min • a1 ≥10 mg/minb • Nor-epinephrine (Levophed) - a1b1 >>b2 • Dopamine - Dopaminergic 0–3 mg/kg/min b 3–10 mg/kg/min a >10 mg/kg/minb • Dobutamine - b1 >> b2a • Isoproterenol ( Isuprel ) - b1 > b2
Conclusion • Removal of pericardial fluid is the definitive and effective therapy for tamponade. • Anesthesia plan is important for the patients with cardiac tamponade. • If general anesthesia is needed, adequate monitors must be setup before induction. • CVS doctors standby is important if emergent drainage was necessary during induction.