Download
1 / 1
20 likes | 173 Views
Acoustic Analysis and Electropalatography (EPG) in the Assessment and Treatment of Children with Intractable Speech Disorders Sara E. Wood James M. Scobbie. Fig. 5 “a cop”. Fig. 8 “a tap”. Fig. 6 “a cap”. Fig. 7 “a coke”. Background

E N D
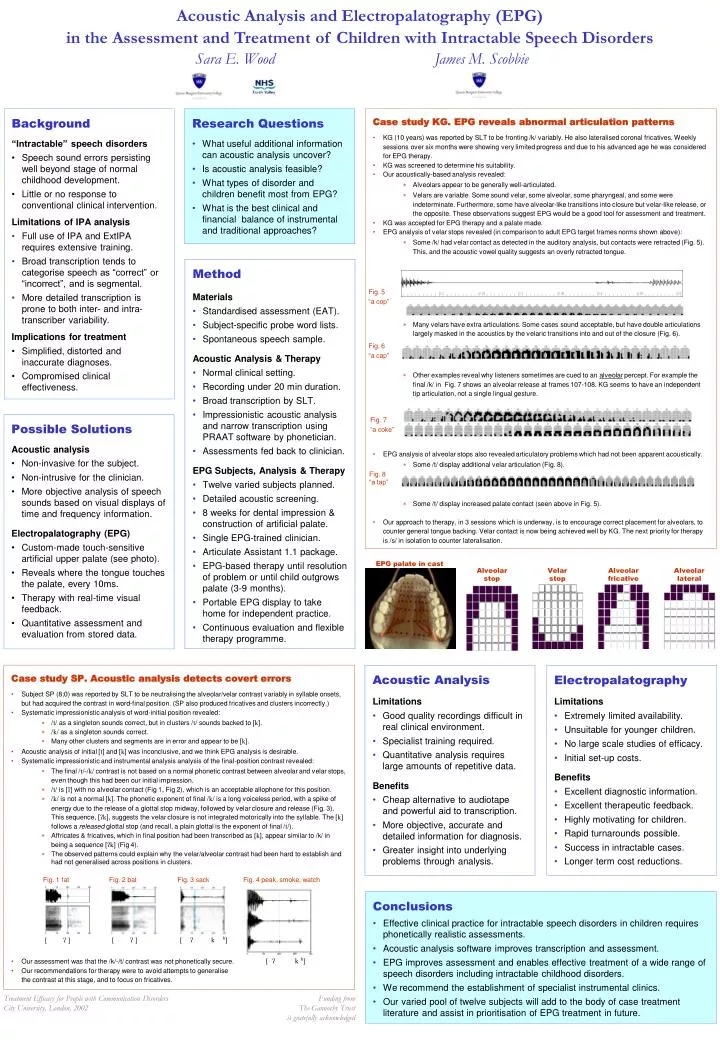
Acoustic Analysis and Electropalatography (EPG)in the Assessment and Treatment of Children with Intractable Speech DisordersSara E. Wood James M. Scobbie Fig. 5 “a cop” Fig. 8“a tap” Fig. 6 “a cap” Fig. 7 “a coke” • Background • “Intractable” speech disorders • Speech sound errors persisting well beyond stage of normal childhood development. • Little or no response to conventional clinical intervention. • Limitations of IPA analysis • Full use of IPA and ExtIPA requires extensive training. • Broad transcription tends to categorise speech as “correct” or “incorrect”, and is segmental. • More detailed transcription is prone to both inter- and intra-transcriber variability. • Implications for treatment • Simplified, distorted and inaccurate diagnoses. • Compromised clinical effectiveness. • Research Questions • What useful additional information can acoustic analysis uncover? • Is acoustic analysis feasible? • What types of disorder and children benefit most from EPG? • What is the best clinical and financial balance of instrumental and traditional approaches? • Case study KG. EPG reveals abnormal articulation patterns • KG (10 years) was reported by SLT to be fronting /k/ variably. He also lateralised coronal fricatives. Weekly sessions over six months were showing very limited progress and due to his advanced age he was considered for EPG therapy. • KG was screened to determine his suitability. • Our acoustically-based analysis revealed: • Alveolars appear to be generally well-articulated. • Velars are variable. Some sound velar, some alveolar, some pharyngeal, and some were indeterminate. Furthermore, some have alveolar-like transitions into closure but velar-like release, or the opposite. These observations suggest EPG would be a good tool for assessment and treatment. • KG was accepted for EPG therapy and a palate made. • EPG analysis of velar stops revealed (in comparison to adult EPG target frames norms shown above): • Some /k/ had velar contact as detected in the auditory analysis, but contacts were retracted (Fig. 5). This, and the acoustic vowel quality suggests an overly retracted tongue. • Many velars have extra articulations. Some cases sound acceptable, but have double articulations largely masked in the acoustics by the velaric transitions into and out of the closure (Fig. 6). • Other examples reveal why listeners sometimes are cued to an alveolar percept. For example the final /k/ in Fig. 7 shows an alveolar release at frames 107-108. KG seems to have an independent tip articulation, not a single lingual gesture. • EPG analysis of alveolar stops also revealed articulatory problems which had not been apparent acoustically. • Some /t/ display additional velar articulation (Fig. 8). • Some /t/ display increased palate contact (seen above in Fig. 5). • Our approach to therapy, in 3 sessions which is underway, is to encourage correct placement for alveolars, to counter general tongue backing. Velar contact is now being achieved well by KG. The next priority for therapy is /s/ in isolation to counter lateralisation. • Method • Materials • Standardised assessment (EAT). • Subject-specific probe word lists. • Spontaneous speech sample. • Acoustic Analysis & Therapy • Normal clinical setting. • Recording under 20 min duration. • Broad transcription by SLT. • Impressionistic acoustic analysis and narrow transcription using PRAAT software by phonetician. • Assessments fed back to clinician. • EPG Subjects, Analysis & Therapy • Twelve varied subjects planned. • Detailed acoustic screening. • 8 weeks for dental impression & construction of artificial palate. • Single EPG-trained clinician. • Articulate Assistant 1.1 package. • EPG-based therapy until resolution of problem or until child outgrows palate (3-9 months). • Portable EPG display to take home for independent practice. • Continuous evaluation and flexible therapy programme. • Possible Solutions • Acoustic analysis • Non-invasive for the subject. • Non-intrusive for the clinician. • More objective analysis of speech sounds based on visual displays of time and frequency information. • Electropalatography (EPG) • Custom-made touch-sensitive artificial upper palate (see photo). • Reveals where the tongue touches the palate, every 10ms. • Therapy with real-time visual feedback. • Quantitative assessment and evaluation from stored data. EPG palate in cast Alveolar stop Velar stop Alveolar fricative Alveolar lateral • Case study SP. Acoustic analysis detects covert errors • Subject SP (8;0) was reported by SLT to be neutralising the alveolar/velar contrast variably in syllable onsets, but had acquired the contrast in word-final position. (SP also produced fricatives and clusters incorrectly.) • Systematic impressionistic analysis of word-initial position revealed: • /t/ as a singleton sounds correct, but in clusters /t/ sounds backed to [k]. • /k/ as a singleton sounds correct. • Many other clusters and segments are in error and appear to be [k]. • Acoustic analysis of initial [t] and [k] was inconclusive, and we think EPG analysis is desirable. • Systematic impressionistic and instrumental analysis analysis of the final-position contrast revealed: • The final /t/-/k/ contrast is not based on a normal phonetic contrast between alveolar and velar stops, even though this had been our initial impression. • /t/ is [] with no alveolar contact (Fig 1, Fig 2), which is an acceptable allophone for this position. • /k/ is not a normal [k]. The phonetic exponent of final /k/ is a long voiceless period, with a spike of energy due to the release of a glottal stop midway, followed by velar closure and release (Fig. 3). This sequence, [k], suggests the velar closure is not integrated motorically into the syllable. The [k] follows a released glottal stop (and recall, a plain glottal is the exponent of final /t/). • Affricates & fricatives, which in final position had been transcribed as [k], appear similar to /k/ in being a sequence [k] (Fig 4). • The observed patterns could explain why the velar/alveolar contrast had been hard to establish and had not generalised across positions in clusters. • Our assessment was that the /k/-/t/ contrast was not phonetically secure. • Our recommendations for therapy were to avoid attempts to generalise the contrast at this stage, and to focus on fricatives. • Acoustic Analysis • Limitations • Good quality recordings difficult in real clinical environment. • Specialist training required. • Quantitative analysis requires large amounts of repetitive data. • Benefits • Cheap alternative to audiotape and powerful aid to transcription. • More objective, accurate and detailed information for diagnosis. • Greater insight into underlying problems through analysis. • Electropalatography • Limitations • Extremely limited availability. • Unsuitable for younger children. • No large scale studies of efficacy. • Initial set-up costs. • Benefits • Excellent diagnostic information. • Excellent therapeutic feedback. • Highly motivating for children. • Rapid turnarounds possible. • Success in intractable cases. • Longer term cost reductions. Fig. 1 fat Fig. 2 bat Fig. 3 sack Fig. 4 peak, smoke, watch • Conclusions • Effective clinical practice for intractable speech disorders in children requires phonetically realistic assessments. • Acoustic analysis software improves transcription and assessment. • EPG improves assessment and enables effective treatment of a wide range of speech disorders including intractable childhood disorders. • We recommend the establishment of specialist instrumental clinics. • Our varied pool of twelve subjects will add to the body of case treatment literature and assist in prioritisation of EPG treatment in future. [ ? ] [ ? k H] [ ? ] [ ? k H] Treatment Efficacy for People with Communication Disorders City University, London, 2002 Funding from The Gannochy Trust is gratefully acknowledged