Immune Disorders
Immune Disorders. Colleen Carter RN, MSN 2014. Nursing Management of Clients with Organ Transplants. Transplant success tied to matching tissue antigens, HLA (Human Leukocyte Antigens) Autograft Allograft Xenograft

Immune Disorders
E N D
Presentation Transcript
Immune Disorders Colleen Carter RN, MSN 2014
Nursing Management of Clients with Organ Transplants • Transplant success tied to matching tissue antigens, HLA (Human Leukocyte Antigens) • Autograft • Allograft • Xenograft • Histocompatibility – ability of cells and tissues to survive transplantation without immunologic interference by the recipient
Host-versus-Graft Transplant Rejection • Complex process involving both antibody-mediated and cell mediated responses • Hyperacute Rejection – Begins immediately to 2-3 days after the transplant and can’t be stopped once it begins • Acute rejection – occurs 4 days to 3 mo post-transplant. Most common rejection and is treatable. • Chronic rejection – occurs from 4 mos to yrs post-transplant. No cure. Once organ cannot function, another transplant is only course.
Treatment of Transplant rejection Maintenance therapy – Ongoing immune suppressants Ex. cyclosporin, Imuran & a corticosteroid (prednisone) Rescue therapy – treats acute rejection. Ex: ALG , murononab-CD3. Most effective during first course of treatment
System Lupus Erythematosus (SLE) • Chronic, multi-system, autoimmune disease • Affects more women than men • Affects more African American women than European American women • SLE thought to be a combination of environmental and genetic factors • Extremely variable in its course and no way to predict its progression
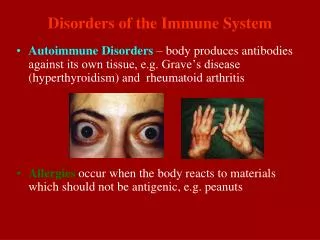
Lupus: Signs and Symptoms • Skin: Butterfly rash • Raynaud’s Phenomenon
Lupus: Signs/Symptoms • Musculoskeletal System • Muscle and joint pain very common with exacerbations and remissions • Arthritis – affects primarily distal joints: hands, wrists, fingers, toes, ankles, knees, etc. • May have tendon involvement and rupture • Knees and hips can have treatment related osteonecrosis from steroid therapy
Lupus: Signs/Symptoms • Cardiac System • Pericarditis - most common cardiac manifestation • Myocarditis • Anemia • Leukopenia • Thrombocytopenia
Lupus: Signs/Symptoms • Respiratory System • Pleuritis – Inflammation of the pleura • Pleural Effusions – Fluid build-up between pleura and chest cavity • Pneumonia
Lupus: Signs/Symptoms • Gastrointestinal/Hepatic Systems • Can affect any area of the GI system as well as pancreas, spleen, or liver • Ex: oral ulcers, peptic ulcers, abdominal pain/N/V/D, pancreatitis, hepatomegaly, GERD, ulcerative colitis
Lupus: Signs/Symptoms • Renal System • Lupus Nephritis – leading cause of death among patients diagnosed with SLE (Lupus) • s/s to monitor for: fluid retention (edema, wt gain), hematuria, proteinuria, changes in urine output, hypertension
Lupus: Signs/Symptoms • Neurologic System • Neuropathies • Psychoses, depression • Seizures, migraine headaches • CNS vasculitis • Peripheral neuropathies CNS Vasculitis
Lupus: Signs/Symptoms • Constitutional Symptoms • Fatigue • Weight changes/loss or gain • Fever • Arthralgias
Lupus: S/S • Psychosocial Issues • Altered body image/poor self-concept • Chronic fatigue/weakness may prevent being as socially active as previously • Fear and anxiety may occur due to the unpredictability of flares or the progression of the disease, necessity of life style changes, etc.
Lupus: Diagnosis • Lab tests: Antinuclear antibody ESR (sed rate) Serum complement Various antibody titers CBC – looking for pancytopenia Specific testing for body system involvement Urinalysis/24 hr urine Diagnostic Imaging: CXR, Hand x-rays, CT OR MRI
Lupus: Treatment • Pharmacologic Management • NSAIDS • Antimalarials (Plaquenil) • Corticosteroid Therapy • Immunosuppressive agents (methotrexate or Imuran)
Lupus: Treatment • Non-pharmacologic Management • Avoid direct exposure to sunlight • Use sunscreen with SPF of 15 or higher • Wide brimmed hat when outside • Some physicians recommend avoiding use of oral contraceptives • Careful skin and hair care with mild soaps/shampoos
Lupus: Important Patient Education • Importance of skin care • Monitor body temp and other warning signs of a flare: increased fatigue, pain, abdominal discomfort, rash, headache, dizziness • Reproductive impact • Avoid exposure to infection • Need to follow treatment plan, including follow-up appointments and prompt reporting of a flare • Preventive health care • Medic Alert bracelet
Rheumatoid Arthritis (RA) • Chronic, progressive, systemic, inflammatory, autoimmune disease that affects joints and other tissues or organ systems. • Most prevalent in European Americans • Affects 0.5% to 1% of the population worldwide; women more frequently than men
RA Pathophysiology • Cause: believed to be genetic and environmental • Autoantibodies (rheumatoid factors) attack healthy tissue, especially synovial membranes, causing inflammation. Immune processes activated • Activation of the inflammatory and immune response damages the synovial membrane.
RA Signs/Symptoms • Onset may be acute and severe (usually precipitated by a stressor such as surgery or an infection) • Or onset may be insidious • Joints primarily affected are hands, wrists, knees and feet • Joint involvement usually bilateral and symmetric. • Disease symptoms described as early or late and joint (articular) or systemic (extra-articular)
RA Signs/Symptoms • Early Disease Manifestations: • Joint stiffness, swelling, pain • Systemic: • Low-grade fever • Fatigue • Weakness • Anorexia • Paresthesias
RA Signs/Symptoms • Late Disease Manifestations • Joint deformities (swan neck and ulnar deviation) • Moderate to severe pain and morning stiffness Swan neck deformity Ulnar deviation
RA Signs/Symptoms • Late Disease Manifestations – Systemic • Osteoporosis • Anemia • Weight loss • Subcutaneous nodules • Peripheral neuropathy • Vasculitis • Pericarditis • Sjogren’s syndrome • Renal disease
RA Diagnosis • Based on patient’s hx, physical assessment, and diagnostic tests • Lab tests: • Rheumatoid factor • ANA • ESR and C-reactive protein • CBC • Synovial fluid exam • X-rays of affected joints
RA Treatment • Surgical Management: • A synovectomy to remove inflamed synovium may be necessary for knee or elbow • Total joint arthroplasty may be necessary for joint deformity and destruction • Arthrodesis (joint fusion) to stabilize joints such as cervical vertebrae, wrists, and ankles.
RA Treatment • Pharmacological Management: • NSAIDS • Antimalarials • Corticosteroids, oral or intra-articular for temporary relief • Disease-Modifying Antirheumatic Drugs (DMARDS) to reduce disease activity: methotrexate, Imuran, Cytoxan or BMR’s: Humira, Enbrel, Remicade
RA Treatment • Non-pharmacological treatment • Plasmapheresis • Balanced program of rest and exercise – energy conservation • Physical and Occupational therapy • Heat and cold • Assistive devices and splints • Balanced nutrition
Scleroderma (Systemic Sclerosis) • Autoimmune disorder of connective tissue • Characterized by hardening(sclero) and thickening of the skin (derma), blood vessels, synovium, skeletal muscles, and internal organs • Approximately 300,000 people in the US have Scleroderma • Affects women more than men by 3:1 • Affects more African Americans than Caucasians
Scleroderma - Pathophysiology • Early stages very similar to SLE – often misdiagnosed • Can be limited or diffuse • May have CREST syndrome: • Calcinosis • Raynaud’s phenomenon • Esophageal dysmotility • Sclerodactyly • Telangiectasia
Scleroderma Signs/Symptoms • Musculoskeletal - Joint pain • GI: Dysphagia and reflux, esophagitis, diarrhea or constipation, abdominal cramping and malabsorption • Skin: Bilateral, symmetric swelling of hands and sometimes feet. After edematous phase, the skin becomes hard and thick. • Facial changes – skin tightening leads to loss of skin lines, appearance of disappearing lips
Scleroderma Signs/Symptoms • Facial skin symptoms: • Tightening of the skin • Disappearing lips • Decreased mobility of eyelids • Evolving process Body image and psychosocial issues
Scleroderma Signs and Symptoms • Cardiovascular: Raynaud’s Syndrome, Myocardial fibrosis, Pericarditis and dysrhythmias • Pulmonary: Lung fibrosis, pulmonary hypertension, exertional dyspnea • Renal – proteinuria, hematuria, hypertension, and renal failure
Scleroderma Diagnosis • ANA: of at least 1:40 • Lab tests/results similar to SLE: ESR – elevated; CBC- may show anemia, RF – elevated in about 30% • Barium swallow – may show esophageal dysmotility • X-ray of hands & wrists – muscle atrophy, osteopenia • No single diagnostic test – overlap with other autoimmune diseases so diagnosis may initially be difficult
Scleroderma Treatment • Corticosteroids & immunosuppressants – tried to slow the progression • Protect hands from the cold • Report fever to the • Skin protection, moisturizer and careful ongoing assessments • Gastric secretion blockers for esophagitis/reflux. Avoid spicy foods, caffeine, alcohol • NSAIDS for joint pain • Be aware that the side effects from many of the pharmacological treatments can worsen symptoms of the disease
Gout • Metabolic d/o characterized by an acute inflammatory arthritis triggered by crystallization of urate within the joints. • May be caused by an inborn error of metabolism or as the result of another disease process or factor; i.e. crash diets, renal insufficiency • Affects approximately 3 million Americans each year, and over twice that man have been affected at some time. • Occurs more often in men. More common in women who are post-menopausal or taking diuretics
Gout • 3 clinical stages • Asymptomatic – not detected unless a uric acid level is checked. • Acute - Extremely painful joint inflammation, usually in the great toe, called podagra • Chronic – After repeated episodes of acute gout, urates are deposited in various other connective tissues: synovial fluids (gouty arthritis); subcutaneous tissue (tophi) and kidneys(can form kidney stones and result in kidney failure)
Gout treatment • Pharmacological Management • Acute Gout: NSAID (Indocin) or ibuprofen; and colchicine. Taken until symptoms subside • Chronic gout: Prevention is key. Zyloprim (allopurinol) lowers uric acid levels. Benemid(probenecid) promotes excretion of uric acid. May be given one or the other or a combination.
Gout treatment • Non-pharmacological Management • Dietary restrictions on high-purine meats (red and organ meats) and seafood (shellfish and oily fish with bones) may be recommended • No alcohol • Avoid aspirin and diuretics • Drink enough fluid to maintain daily urine output of 2000 mL or more
Lyme Disease • Most common tick-borne illness in North America • Carried by the infected deer tick (black-legged tick) • Occurs most often in children and young adults living in rural areas • Risk factors: Spending time in wooded or grassy areas Having exposed skin Not removing ticks promptly or properly
Lyme Disease: Pathophysiology • After an incubation period of 3-30 days after the bite, the spirochete migrates outward into the skin • Forms a characteristic erythema migrans (bull’s eye rash) • May spread to other skin sites, organs, or nodes
Lyme Disease: Signs/Symptoms • Stage I: • Skin: Bull’s eye rash • Musculoskeletal: pain and stiffness in muscles and joints • Constitutional: flu-like symptoms, fever, chills, fatigue, body aches • If not treated or treatment is unsuccessful, progresses to Stage II
Lyme Disease Signs/Symptoms • Stage II: • Migratory musculoskeletal pain and swelling; especially in the knees • Carditis with dysrhythmias, dyspnea, palpitations • CNS disorders: meningitis, Bell’s palsy, numbness or weakness in limbs, impaired muscle movement • If not diagnosed and treated can progress to Stage III
Lyme Disease Signs/Symptoms • Stage III (months to years after the tick bite) • Chronic recurrent arthritis • Chronic fatigue • Cardiac complications • Thinking/memory issues
Lyme Disease: Treatment • Antibiotic therapy: doxycycline, tetracycline, amoxicillin, cefuroxime, erythromycin. May be given for 3-4 weeks • Aspirin or another NSAID for relief of arthritic symptoms • May need assistive devices (splints/crutches) • Prevention is the Key
Preventing Lyme Disease • When walking in wooded or grassy areas: • Wear long pants tucked into socks, long sleeves, hat, gloves, shoes • Use insect repellents (10-30% DEET) • Check yourself, your children and your pets for ticks • Remove a tick with tweezers by pulling straight out. Clean with alcohol other antiseptic.
Fibromyalgia • Common rheumatic pain syndrome with wide-spread musculoskeletal pain, stiffness, and tenderness • Women affected 9 times more often than men • Genetic and environmental factors are thought to contribute • Requires a hx of widespread pain in all 4 quadrants of the body for a minimum duration of 3 months and pain in at least 11 of 18 trigger points
Fibromyalgia Signs/Symptoms • Fatigue, moderate to severe • Sleep disorders • Problems with cognitive function (Fibro Fog) • Irritable Bowel Syndrome • Headaches and migraines • Anxiety and depression • Environmental sensitivities
Fibromyalgia Treatment • Pharmacological Management is symptomatic: • 3 drugs approved as of 2009 to reduce pain levels and improve sleep: Lyrica, Cymbalta, and Savella • Tricyclic antidepressants such as amitryptyline may help with pain and sleep as well • SSRI’s - treat depression and anxiety
Fibromyalgia Treatment • Non-pharmacological Management • Physical therapy • Regular exercise routine • Alternative therapies: Massage, acupuncture, chiropractic, yoga • Stress management • Therapy to assist with depression/anxiety