Download
1 / 68
740 likes | 1.24k Views
Chapter : 37 Hypothalamic & pituitary hormones. Anterior pituitary hormones & their hypothalamic regulators. Anterior pituitary hormones. Are essential for the regulation of growth and development, reproduction, responses to stress, and intermediary metabolism

E N D
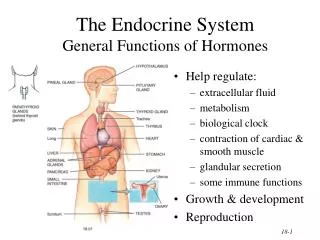
Anterior pituitary hormones • Are essential for the regulation of growth and development, reproduction, responses to stress, and intermediary metabolism • Within this tissue are specialised cells such as corticotrophs, lactotrophs (mammotrophs), somatotrophs, thyrotrophs and gonadotrophs, which secrete hormones that regulate different endocrine organs of the body • Their synthesis and secretion are controlled by hypothalamic hormones and by hormones from the peripheral endocrine organs (negative feedback control)
+ + - - Stimulus Hypothalamus Hypothalamic hormone -ve feedback Anterior pitutary gland Anterior pituitary hormone Endocrine gland Hormone Target tissue Feedback mechanisms Response
Anterior pituitary hormones • Hypothalamic hormones somatostatinand gonadotrophin-releasing hormone are used therapeutically, the rest being used for diagnostic tests or as research tools
Anterior pituitary hormones • A large number of disease states, as well as a diverse group of drugs, also affect their secretion • Knowledge of the levels of the pituitary signal hormone and the target hormone allows the clinician to identify the site of the endocrine disorder. • Endocrine deficiency states can be divided into: primary, secondary and tertiary
Anterior pituitary hormones • In primary hypofunction, the production of the target endocrine hormone will be impaired; however, the hypothalamus and pituitary will sense the diminished feedback inhibition and the anterior pituitary gland will secrete higher than normal levels of the signal hormone • In secondary hypofunction, both the signal hormone and the target hormone will be below the normal range
Anterior pituitary hormones • Hormone excess similarly can result either from: • Primary disorders at the level of the target endocrine glands (e.g., a hyperfunctioning tumor of the adrenal cortex that oversecretes cortisol) • Secondary disorders at the level of the pituitary gland (e.g., a pituitary corticotrope adenoma that oversecretes corticotropin, the predominant stimulator of adrenal glucocorticoid biosynthesis)
I. Growth hormone (Somatotropin, GH) • The hypothalamus secretes two hormones that regulate GH: • GH-releasing hormone (GHRH) • Somatostatin (SST) • GH is released in a pulsatile manner, with the highest levels occurring during sleep • GH is required during childhood and adolescence for attainment of normal adult size • It has an important role throughout life on lipid and CHO metabolism
Physiological Effects of Growth Hormone • Many physiologic effects of GH are exerted directly at its target: GH acts directly on adipocytes to increase lipolysis and on hepatocytes to stimulate gluconeogenesis • The anabolic & growth-promoting effects are mediated indirectly through an increase in the production of insulin-like growth factor 1 (IGF-1)in the liver, bone, cartilage, muscle, and the kidney
Hypothalamus + + + + - - - GHRH Somatostatin Anterior pitutary gland GH Liver IGF-1 Lipolysis ↓ glucose uptake by muscles Growth prmoting actions: ↑cell division ↑protein synthesis ↑bone growth
Physiological Effects of Growth Hormone • The main effect of growth hormone (and its analogues) is to stimulate normal growth in conjunction with other hormones secreted from the thyroid, the gonads and the adrenal cortex • GH stimulates longitudinal bone growth until the epiphyses close—near the end of puberty • In both children and adults, GH has anabolic effects in muscle and catabolic effects in lipid cells that shift the balance of body mass to an increase in muscle mass and a reduction in central adiposity
Pathophysiology of Growth Hormone • Distinct endocrine disorders result from either excessive or deficient GH production • Children with GH deficiency (pituitary dwarfism) present with short stature often with mild adiposity, delayed bone age, and a low age-adjusted growth velocity
Pathophysiology of Growth Hormone • GH deficiency in adults is associated with decreased muscle mass and exercise capacity, decreased bone density, impaired psychosocial function, and increased mortality from CV causes, probably secondary to deleterious changes in fat distribution, increases in circulating lipids, and increased inflammation
Pathophysiology of Growth Hormone • An excessive production of growth hormone in children results in gigantism. It occurs due to GH-secreting adenoma before the long bone epiphyses close • An excessive production in adults, which is usually the result of a benign pituitary tumour, results in acromegaly, which is characterized by abnormal growth of cartilage and bone tissue, and many organs including skin, muscle, heart, liver, and GIT
GH preparations • Somatropin refers to the many GH preparations whose sequences match that of native GH: accretropin, genotropin, humatrope, norditropin, nutropin, omnitrope, saizen, serostim, tevtropin, valtropin, and zorbtive • GH is administered subcutaneously • To match the usual pattern of secretion, GH typically is administered at bedtime
Clinical uses • Treatment of growth hormone deficiency (dwarfism) • Children with other conditions associated with short stature caused by factors other than GH deficiency: • Turner's syndrome • Noonan's syndrome • Prader-Willi syndrome • Chronic renal insufficiency in pediatric patients • Children born small for gestational age • Children with idiopathic short stature1
Other uses of GH • GH affects many organ systems and also has a net anabolic effect. It is approved for the treatment of: • Wasting in patients with AIDS • Short bowel syndrome • GH is a popular component of anti-aging programs • Used by athletes to increase lean body mass and athletic performance (banned by Olympic committee) • Bovine growth hormone (rbGH) in dairy cattle to increase milk production
Insulin-like growth factor 1 (IGF-1) • Two preparations are FDA-approved: • Mecasermin: recombinant human IGF-1 • Mecaserminrinfabate: is a complex hIGF-1 and recombinant human insulin-like growth factor-binding protein-3 (rhIGFBP-3) • Mecasermin is administered SC
Insulin-like growth factor 1 (IGF-1) • Mecasermin is FDA-approved for: • Patients with impaired growth secondary to mutations in the GH receptor or postreceptorsignaling pathway • Patients with GH deficiency who develop antibodies against GH that interfere with its action • Patients with IGF-1 gene defects that lead to primary IGF-1 deficiency • Mecaserminrinfabate is currently approved for severe insulin resistance, muscular dystrophy, and HIV-related adipose redistribution syndrome
Growth hormone antagonists • Pegvisomantis a GH receptor antagonist • It binds to the GH receptor but does not activate or stimulate IGF-1 secretion • Approved by the FDA for the treatment of acromegaly • Administered SC • Based on serum IGF-1 levels, the dose is titrated at 4- to 6-week intervals
II. Growth hormone-releasing hormone (GHRH, somatorelin) • It is a peptide with 40-44 amino acid residues • It stimulates the synthesis & release of growth hormone (GH) from the anterior pituitary • Sermorelin, is a GHRH analogue, was withdrawn from the U.S. market in late 2008
III. Somatostatin (GHIH, SRIH) • Somatostatin is found in the hypothalamus, other parts of the CNS, the pancreas, and other sites in the GIT • In the pituitary, somatostatin binds to distinct receptors, SSTR2 and SSTR5, which suppress GH & TSH release • It inhibits the release of GH, TSH, glucagon, insulin, and gastrin
Somatostatin (GHIH, SRIH) • Exogenous Somatostatin has limited therapeutics usefulness: • Short duration of action (t1/2 = 1-3 minutes) • Multiple effects on many secretory systems • Longer-acting somatostatin analogs have been developed: Octreotide & Lanreotide
Octreotide • The most widely used somatostatin analog • It has a longer half-life (half-life ~ 90 mins), and duration of action ~ 12 hrs • It is 45 times more potent that somatostatin in inhibiting GH with reduced effect on pancreatic β-cells (hyperglycemia rarely occurs) • Octreotide is administered SC three times daily • A long-acting, slow-release form is administered IM every 4 week, typically to patients who have tolerated and responded to the shorter-acting formulation
Octreotide- Clinical uses • Treat/reduce symptoms of hormone-secreting tumors (e.g. acromegaly, tumors producing vasoactive intestinal peptide (VIPomas)) • Acute control of bleeding from esophageal varices • Perioperative prophylaxis in pancreatic surgery • Thyrotropeadenomas that oversecrete TSH who are not good candidates for surgery (DOC): Octreotidehas significant inhibitory effects on TSH secretion
Octreotide- Clinical uses • Modified forms of octreotidelabeled with indium or technetium have been used for diagnostic imaging of neuroendocrine tumors such as pituitary adenomas and carcinoids (OCTREOSCAN) • Modified forms labeled with emitters such as 90Y have been used in selective destruction of SST2 receptor-positive tumors
Lanreotide • Long-acting octapeptide analog of somatostatin that causes prolonged suppression of GH secretion when administered IM • Efficacy comparable to that of the long-acting formulation of octreotide, but its duration of action is shorter (it is administered either at 10- or 14-day intervals) • Lanreotideautogelis supplied in prefilled syringes and administered by deep Sc injection once every 4 weeks. It provides more uniform drug levels than the depot formulation of octreotide
II. The Gonadotropins • Gonadotropins: • Luteinizing hormone (LH) • follicle-stimulating hormone (FSH) • chorionic gonadotropin (hCG) • LH and FSH are synthesized and secreted by gonadotropes cells in the anterior pituitary • hCG is produced by the human placenta and excreted into the urine • Production is stimulated by pulses of GnRH secreted by hypothalamus and by feedback effects of the gonadal hormones
Mechanism of action • The actions of LH and hCG on target tissues are mediated by the LH receptor; those of FSH are mediated by the FSH receptor • The gonadotropins and hCG exert their effects through G protein-coupled receptors • The FSH and LH receptors couple to Gs to activate the adenylyl cyclase/cyclic AMP pathway
Physiological effects of Gonadotropin • The male: • LH acts on testicular Leydig cells to stimulate the de novo synthesis of androgens, primarily testosterone • FSH is the primary regulator of spermatogenesis. It acts on the Sertoli cells to stimulate the production of proteins and nutrients required for sperm maturation
Physiological effects of Gonadotropin • The female: • The actions of FSH and LH are more complicated • A coordinated pattern of FSH and LH secretion during the menstrual cycle is required for normal follicle development, ovulation, and pregnancy • FSH stimulates the growth of developing ovarian follicles and induces the expression of LH receptors on theca and granulosa cells
Physiological effects of Gonadotropin • The female: • LH acts on the theca cells to stimulate the de novo synthesis of androgens, whereas FSH stimulates the conversion by granulosa cells of androgens to estrogens • hcG is a placental protein that stimulates the ovarian corpus luteum to produce progesterone and maintain the placenta in females during pregnancy
Clinical Uses • Diagnostic Uses of Gonadotropins • Diagnosis of Pregnancy: • Commercial pregnancy kits (qualitative assay) which can be detected in maternal urine
Clinical Uses • Diagnostic Uses of Gonadotropins • Diagnosis of Pregnancy: • Quantitative measurements of plasma hCG concentration by immunoassay can indicate whether pregnancy is proceeding normally and can help to detect the presence of an ectopic pregnancy, hydatidiform mole, or choriocarcinoma • Such assays also are used to follow the therapeutic response of malignancies that secrete hCG, such as germ cell tumors
Clinical Uses • Therapeutic Uses of Gonadotropins • Ovulation induction: in women with anovulation that is secondary to hypogonadotropichypogonadism, polycystic ovary syndrome, obesity, and other causes • Controlled ovarian hyperstimulation • Male infertility
III. Gonadotropins releasing hormone (GnRH, gonadorelin) • Decapeptide secreted by neurons in the hypothalamus that control the release of gonadotropins FSH & LH • The intermittent/ pulsatile release of GnRH is crucial for the proper synthesis and release of the gonadotropins
III. Gonadotropins releasing hormone (GnRH, gonadorelin) • The continuous/ sustained/ nonpulsatile administration of GnRH leads to desensitization and down-regulation of GnRH receptors on pituitary gonadotropes • This inhibits the release of FSH and LH by the pituitary in both women and men, resulting in hypogonadism
Clinical uses • Pulsatile intravenous administration of gonadorelin every 1–4 hours stimulates FSH and LH secretion • Continuous administration of gonadorelin or its longer-acting analogs produces a biphasic response: • Flare (first 7–10 days): increase concentrations of gonadal hormones • The continued presence of GnRH results in an inhibitory action (drop in the concentration of gonadotropins and gonadal steroids)
1. Stimulation • Female Infertility: pulsatile GnRH is less likely than gonadotropins to cause multiple pregnancies and the ovarian hyperstimulation syndrome, the inconvenience and cost associated with continuous use of an intravenous pump and difficulties obtaining gonadorelin are barriers to pulsatile GnRH • Male Infertility: pulsatile gonadorelin for infertility in men with hypothalamic hypogonadotropic hypogonadism
1. Stimulation • Diagnosis of LH responsivness (delayed puberty): to determine whether delayed puberty in a is due to constitutional delay or to hypogonadotropic hypogonadism
2. Suppression • Controlled ovarian hyperstimulation, such as IVF, to suppress an endogenous LH surge • Palliative therapy of hormonally responsive tumors (e.g., prostate cancer) • Suppress steroid-responsive conditions such as endometriosis and uterine Fibroids • Treatment of central precocious puberty
GnRH receptor antagonists • Agents: Ganirelix, cetrorelix, anddegarelix • Competitive antagonists of GnRH receptors that inhibit the secretion of FSH and LH in a dose-dependent manner • They do not induce an initial hypersecretion of gonadotropins but instead cause an immediate and rapid, reversible suppression of gonadotropin secretion
Clinical uses • Suppression of Gonadotropin Production: preventing the LH surge during controlled ovarian hyperstimulation • Advanced Prostate Cancer (Degarelix)
IV. Prolactin • Prolactin is a peptide hormone secreted from the anterior pituitary by lactotroph (mammotroph) cells • Its structure resembles that of GH • Prolactin is unique among the anterior pituitary hormones in that hypothalamic regulation of its secretion is predominantly inhibitory • Prolactin production is inhibited by the catecholamine dopamine acting through the D2 subtype of dopamine receptor
Prolactin secretion and actions. Prolactin is the only anterior pituitary hormone for which a unique stimulatory releasing factor has not been identified. Thyrotropin-releasing hormone (TRH), however, can stimulate prolactin release and dopamine can inhibit it. Suckling induces prolactin secretion, and prolactin affects lactation and reproductive functions but also has varied effects on many other tissues. Prolactin is not under feedback control by peripheral hormones
IV. Prolactin • Prolactin primary function is to stimulate and maintain of lactation: it plays an important role in inducing growth and differentiation of the ductal and lobuloalveolar epithelium • It decreases sexual drive and reproductive function • No preparation of prolactin is available for use in prolactin-deficient patients • Dopamine agonists are used to inhibit prolactin secretion in patients with symptomatic hyperprolactinemia
IV. Prolactin • Prolactin receptors are widely distributed cell surface receptors that belong to the cytokine receptor superfamily and thus share structural similarity with the receptors for GH
Dopamin agonists • Dopamine agonists suppress prolactin release via activation of D2 dopamine receptors • Agents: • Ergot derivatives: bromocriptine, cabergoline, & pergolide • Non-ergot derivative: Quinagolide • All available dopamine agonists are active as oral preparations