Download
1 / 24
240 likes | 250 Views
This study investigates the association of missed metastases on MRI with technical imaging factors and radiologist qualifications to improve pediatric cancer imaging and metastasis detection.

E N D
Analyzing Misdiagnosed Metastasis on Imaging Studies Jacqueline Angel, MD Julie Harreld, MD St. Jude Children’s Research Hospital ASNR 2016 Annual Meeting May 23-26, 2016 Control #: 2288 Poster #: eP-179
Disclosures Nothing to disclose
Outline • Background • Purpose • Methods • Results • Conclusion
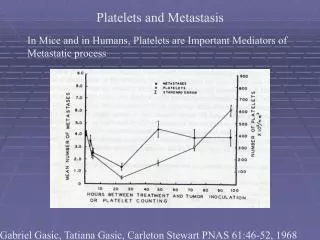
Background • Children are subject to ependymomas and embryonal tumors (primitive neuroectodermal tumor, medulloblastoma, atypical teratoid rhabdoid tumor, and pineoblastoma) of the CNS, which frequently metastasize via the CSF. Medulloblastoma Post-contrast axial T1 Primitive Neuroectodermal Tumor (PNET) Post-contrast axial T1 Atypical Teratoid Rhabdoid Tumor (ATRT) Post-contrast axial T1 Pineoblastoma Post-contrast sagittal T1 Ependymoma Post-contrast sagittal T1
Background • Accurate detection of leptomeningeal metastasis is critical for appropriate risk stratification and treatment of childhood CNS tumors. • MRI findings correlate better with survival than CSF analysis, but leptomeningeal metastases may be missed or misdiagnosed on examinations not optimized for pediatric cancer imaging.
Background:Leptomeningeal Metastasis • Dissemination of tumor via CSF along surfaces of brain and spinal cord • MRI appearance • T1: sulci may appear normal or subtly irregular • T1 +Contrast: may or may not enhance • T2: most are hyperintense • FLAIR: nodular or confluent hyperintensity in sulci and cisterns • FLAIR +Contrast: increased conspicuity of leptomeningeal metastases • T2 hyperintense • Gadolium enhancement • CSF suppressed • Non-visualization of vessels in sulci
Leptomeningeal Metastasis: Intracranial T1 + Contrast FLAIR + Contrast T2 T2 FLAIR Metastatic right frontal PNET (outlined). Extensive non-enhancing leptomeningeal metastases with nodular irregularity of sulci on axial T1WI +Contrast and axial T2WI, and filling of sulci on T2 FLAIR, are much more obvious on axial FLAIR +Contrast with fat saturation.
Leptomeningeal Metastasis: Spine T1WI +Contrast show nodular and plaque-like enhancing medulloblastoma metastases along the spinal cord.
Purpose To investigate the association of missed metastases on MRI with technical imaging factors and radiologist qualifications to promote improvements in pediatric cancer imaging and metastasis detection.
Methods • Retrospectively reviewed reports for outside (OSH) and in-house brain and spine MRIs performed within 35 days of each other for 86 children presenting to our institution between 1/1/2011 and 12/31/2012 with leptomeningeal-seeding brain tumors • Contemporaneous CSF and/or in-house MRI were considered gold standard for metastasis detection • OSH and in-house MRI techniques and radiologist qualifications were compared for cases of missed/misdiagnosed metastases
Methods • In-house spine imaging protocol (30 minutes total): • Sagittal T1 +Contrast • Upper and Lower sections • Two 3mm (0 gap) acquisitions at each level, offset by one slice • Interleave two acquisitions 3mm slices with 1.5mm OVERLAP • No gap, reducing chance of missing metastasis • Increase confidence of diagnosis • Axial VIBE T1 +Contrast • 3D acquisition, 3mm (0 gap) reconstructions • No CSF pulsation • Sagittal T2 • Upper and Lower • Detect non-enhancing metastases
Methods • In-house brain imaging protocol (42 minutes total): • Sag T1 (4mm, 0 gap) • Ax T2 (4mm, 0 gap) • Ax T1 (4mm, 0 gap) • Ax T1 +Contrast (4mm, 0 gap) • T1 subtractions • Cor T1 +Contrast (4mm, 0 gap) • Sag 3D T1 +Contrast (1mm isotropic) • Ax FLAIR +Contrast (4mm, 0 gap)
Results • 31/86 patients (36%) had leptomeningeal metastases (13 brain, 3 spine, 15 both) by initial in-house MRI ± CSF. • Of these, 10/31 (32%) had metastases previously undiagnosed by OSH MRI of brain (n=3), spine (n=4), or both (n=3).
Results • Contributing factors – Brain MRI: • 2/6 had no DWI • 5/6 had no post-contrast FLAIR
Results: DWI FLAIR +Contrast T1 +Contrast Axial FLAIR at an OSH of a 33 mo male with ATRT does not demonstrate leptomeningeal metastasis. No DWI sequence was performed at the facility. In-house MRI performed 2 weeks later shows no focus of enhancement to suggest leptomeningeal metastasis. However, DWI images reveal hypercellular metastases with diffusion restriction in the left frontal horn and right Sylvian fissure (arrows). DWI
Results: Post-contrast FLAIR • Leptomeningeal metastases are best visualized on post-contrast FLAIR with fat saturation, given its T1 and T2 contributions • CSF nulling increases conspicuity of metastases in the sulci, when compared to T2 Axial T1 post-contrast and FLAIR post-contrast, in-house. Non-enhancing leptomeningeal metastases clearly fill the sulci. T1 post-contrast and FLAIR without contrast, OSH. In this 16 yo male with a PNET, metastases are not identified.
Results: Reading Radiologist Normal infundibular recess on T1 post-contrast MRI. In-house sagittal T1 post-contrast MRI, however, shows an enhancing lesion in the infundibular recess (arrow). The OSH reading radiologist did not identify an infundibular recess metastasis, which was present, on T1 post-contrast, DWI, or ADC MR images in this 4 yo female with medulloblastoma.
Results • Contributing factors – Spine MRI: • 3/7 had no spine MRI at the outside facility • 1 out of the 4 imaged spines utilized a TSE for axial T1 post-contrast MR images, which is susceptible to CSF pulsation artifact • 2/4 had no sagittal T2 sequence
Results: Sagittal T2 and TSE Sequences In-house These metastases of an ATRT are best seen on sagittal T2 MRI, which was not performed at the OSH. In-house T1 VIBE +Contrast 3D acquisition, also, shows the lesions (arrows). OSH In-house T2 In-house and OSH T1 post-contrast MRI do not demonstrate the metastases. Additionally, axial T1 post-contrast images at the OSH were performed as a TSE sequence, resulting in CSF pulsation artifact obscuring the metastases (arrow). T1 +Contrast T1 TSE +Contrast T1 VIBE +Contrast
Results: Gap • Unlike in-house examinations, all outside studies with missed metastases had gaps between slices on one or more sequences. In-house 3 mm slices 0 mm gap • Use of thin axial images (3 mm) with no gap permits lesion visibility on 3 consecutive axial images on an in-house study, increasing confidence of diagnosis compared to OSH study using thick slices and a gap. OSH 6 mm slices 2 mm gap
Results: Gap Slice thickness: 3 mm Gap: 0 mm Overlap: 1.5 mm Slice thickness: 4 mm Gap: 1.5 mm OSH In-house Differences in slice thickness and gap between slices can limit evaluation for metastases, as seen in this metastatic pineoblastoma on in-house and OSH sagittal post-contrast T1WI.
Results • In-house and OSH false positive rates were identical (2/55 or 4%) • 4 of 11 (36%) of the missed/misdiagnosed cases with identifiable OSH radiologists had a CAQ in neuroradiology, compared to 3 out of 5 (60%) in-house neuroradiologists
Conclusion Standardization and optimization of MRI technique, and interpretation by subspecialty-trained neuroradiologists, could promote more accurate pediatric CNS cancer detection and risk assessment.
References Engelhard HH, Corsten LA. Leptomeningeal metastasis of primary central nervous system (CNS) neoplasms. Cancer Treat Res 2005;125:71-85. Estlin E, Gilbertson RJ, Wynn R. Pediatric hematology and oncology : scientific principles and clinical practice. Chichester, West Sussex, UK ; Hoboken, NJ: Wiley-Blackwell; 2010. Fangusaro J, Van Den Berghe C, Tomita T, et al. Evaluating the incidence and utility of microscopic metastatic dissemination as diagnosed by lumbar cerebro-spinal fluid (CSF) samples in children with newly diagnosed intracranial ependymoma. J Neurooncol 2011;103:693-698. Fukuoka H, Hirai T, Okuda T, et al. Comparison of the added value of contrast-enhanced 3D fluid-attenuated inversion recovery and magnetization-prepared rapid acquisition of gradient echo sequences in relation to conventional postcontrast T1-weighted images for the evaluation of leptomeningeal diseases at 3T. AJNR Am J Neuroradiol. May 2010;31(5):868-873. Griffiths PD, Coley SC, Romanowski CA, Hodgson T, Wilkinson ID. Contrast-enhanced fluid-attenuated inversion recovery imaging for leptomeningeal disease in children. AJNR Am J Neuroradiol. Apr 2003;24(4):719-723. Kremer S, Abu Eid M, Bierry G, et al. Accuracy of delayed post-contrast FLAIR MR imaging for the diagnosis of leptomeningeal infectious or tumoral diseases. J Neuroradiol. Dec 2006;33(5):285-291. Maroldi R, Ambrosi C, Farina D. Metastatic disease of the brain: extra-axial metastases (skull, dura, leptomeningeal) and tumour spread. Eur Radiol 2005;15:617-626. Osborn AG. Osborn’s Brain: Imaging, Pathology, and Anatomy. Amirsys; 2013. Pang J, Banerjee A, Tihan T. The value of tandem CSF/MRI evaluation for predicting disseminated disease in childhood central nervous system neoplasms. J Neurooncol 2008;87:97-102. Poltinnikov IM, Merchant TE. CSF cytology has limited value in the evaluation of patients with ependymoma who have MRI evidence of metastasis. Pediatric blood & cancer 2006;47:169-173. Terterov S, Krieger MD, Bowen I, et al. Evaluation of intracranial cerebrospinal fluid cytology in staging pediatric medulloblastomas, supratentorial primitive neuroectodermal tumors, and ependymomas. J Neurosurg Pediatr 2010;6:131-136.