Download
1 / 17
180 likes | 629 Views
Keeping the ‘Normal’ in Normal Birth. Interdisciplinary Panel Discussion November 30 th , 2006. ‘Normal’ Birth: A Problematic Notion. Wide range of normal amongst labouring women Notion of normal has different meanings in different contexts WHO Definition

E N D
Keeping the ‘Normal’ in Normal Birth Interdisciplinary Panel Discussion November 30th, 2006
‘Normal’ Birth: A Problematic Notion • Wide range of normal amongst labouring women • Notion of normal has different meanings in different contexts • WHO Definition • Obstetric Normality in Active Management of Labour • Intervention has become the norm in contemporary culture
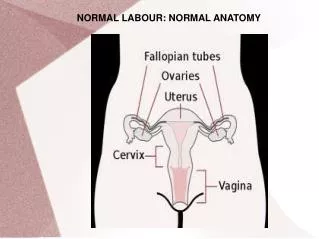
WHO Definition of Normal Birth: • Spontaneous in its onset • low-risk at the start and throughout labour and delivery. • Baby is born spontaneously in the vertex position between 37 and 42 gestation • Following birth both mother and infant are in good condition.
Normal Progression in Active Management of Labour • Strict diagnostic criteria for labour onset • Artificial Rupture of the Membranes (ARM) if dilatation not maintained at rate of l cm/ hr • Augmentation with synthetic oxytocin if dilatation not increasing at this same rate • Charting of labour progress– the partogram. • The provision of customized childbirth education & continuous 1 on 1 support*
Intervention As Normal: Physiologic Birth:The spontaneous head-first delivery of a single baby without employment of narcotics, entinox or epidurals, synthetic hormones-induction or augmentation of labor, artificial rupture of the membranes or episiotomy. (Midwifery) Physiologic birthrate in Nova Scotia:4 • 1.75% for first time mothers • 5% for women having their second or subsequent baby
Birth Intervention Menu • Continuous Electronic Fetal Monitoring • IV Drip • Catheterization • Epidurals, Narcotics, Entinox • Labour Induction • Artificial Rupture of Membranes • Labour Augmentation • Operative Assisted Delivery • Caesarean Sections
Intervention Menu: The Gaps • 1 to 1 Continuous caregiver support (Midwife/ Douala/ Other trained birth attendant) • Consistent Information, Education and Support re Non-pharmacological Pain Relief Methods • Nourishment
Interventions: The Cascade Effect • Cascade: A succession of things…each of which activates, effects, or determines the next • Understanding the Cascade of Interventions
The Cascade of Intervention6 • Directional Relationships highlighted in this diagram have all been established in scientific literature. • To interpret the diagram begin with an intervention of interest and follow arrows from that point.
Caesarean Sections Infant Risks: • Breathing Problems • Low Apgar Scores • Fetal Injury • Increased Neonatal Deaths & NICU Admissions • Premature Birth • Lower Breastfeeding Initiation • Increased Asthma Incidence • Higher Stillbirth Rate amongst women with previous C/S Maternal Risks: • Operative & Post-Op complications: e.g. bleeding, clots, infections, transfusions • Increased pain, length of recovery, hospital stay and re-admission • Respiratory complications • Secondary infertility • Ectopic pregnancy • Placental abruption/ adherence problems • uterine rupture before and during labor • Need for further surgeries (e.g. Hysterectomy, bladder repairs)
Caesarean Sections: The Financial Costs9 • Average Cost of Vaginal Delivery Without Complications in 2002/2003: $2700 • Average Cost of Caesarean Delivery Without Complications in 2002/2003: $4600
Best Practice Guidelines • The World Health Organization (WHO) states that no region in the world is justified in having a cesarean rate greater than 10 to 15 percent.10
References 1. Kaufman KJ, Effective control or effective care, (roundtable debate: active management part 2) Birth, 1993; 20(3): 150-61 2. World Health Organisation (1996). Care in Normal Birth: A practical guide. www.who.int/reproductive-health/publications/MSM_96_24/MSM_96_24_Chapter1.en.html 3. Thornton, J.G (1996). Active management of labour. BMJ, 313: 378. http://www.bmj.com/cgi/content/full /313/7054/378 4. Source: The Reproductive Care Program of NS 5. The second national U.S. Listening to Mothers® survey (2006). http://www.marketwire.com/mw/release_html_b1?release_id=175714 6. Cascade of Intervention: http://www.acegraphics.com.au/parents/obstetric/diagram.html 7. Canadian Institute for Health Information (2004) Giving Birth In Canada: A Regional Profile. http://secure.cihi.ca/cihiweb/products/GBC2004_regional_e.pdf 8. Prepared By the NL Centre for health Information, November 8th, 2006 9. Canadian Institute For Health Information (2006) Giving Birth in Canada: The Costs. http://secure.cihi.ca/cihiweb/products/Costs_Report_06_Eng.pdf 10. WHO Guidelines for Caesarean Sections - http://www.childbirth.org/section/CSFact.html