PROSTATIC DISORDERS
PROSTATIC DISORDERS. Douglas F. Milam, M.D. Department of Urologic Surgery Vanderbilt University Nashville, Tennessee. Common Prostatic Diseases. Benign Prostatic Hyperplasia Acute Prostatitis Chronic Prostatitis Adenocarcinoma of Prostate. Prostatic Zones.

PROSTATIC DISORDERS
E N D
Presentation Transcript
PROSTATIC DISORDERS Douglas F. Milam, M.D. Department of Urologic Surgery Vanderbilt University Nashville, Tennessee
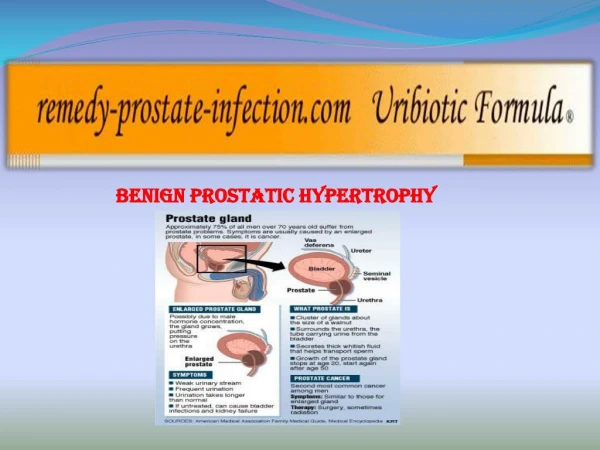
Common Prostatic Diseases • Benign Prostatic Hyperplasia • Acute Prostatitis • Chronic Prostatitis • Adenocarcinoma of Prostate
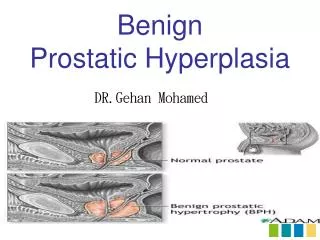
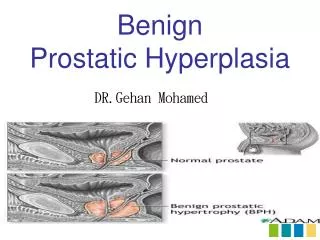
Prostatic Zones • The prostate consists of three distinct zones. • Obstruction is caused by growth of the blue transition zone shown here • 70% of prostatic cancers occur in the yellow peripheral zone
Risk of Microscopic BPH Berry, Coffey, Walsh and Ewing, J Urol, 132:474,1984.
Diagnosis of BPH • AUA symptom score • Digital Rectal Exam (DRE) • Urinary flow rate • Urodynamic testing • Post-void urine residual
Implications of the AUA Symptom Score • Patients with mild symptoms (<8) should not be offered either medical or surgical treatment • Those with moderate symptoms should be offered medical therapy or in office minimally invasive thermal therapy as initial treatment • Either medical or surgical treatment is appropriate initial treatment for severely symptomatic individuals (AUA SS >19)
MTOPS Study • Largest and longest BPH trial • 3,047 men age 50 and above • AUA SS 8-30 • Randomized to 4 groups • Mean F/U of 4.5 years • Extensive quarterly F/U • McConnell, et al, Long-term effects of doxazosin, finasteride, and combination therapy on the clinical progression of BPH, New England Journal of Medicine. 172:1792-1799,2004 Nov.
MTOPSPrimary Research Question • To Determine if Medical Therapy Prevents or Delays the Clinical Progression of BPH as defined by one of the following: • Acute urinary retention (AUR) • Renal insufficiency due to BPH (> 50% rise in baseline serum creatinine & > 1.5 mg/dl) • Recurrent UTI or urosepsis • Incontinence (socially unacceptable) • ≥ 4 - Point Rise in Baseline AUA Symptom Score confirmed within 2 - 4 weeks
Cumulative Incidence of >4-Pt AUA Rise 2 5 2 0 1 5 1 0 5 0 0 . 0 0 . 5 1 . 0 1 . 5 2 . 0 2 . 5 3 . 0 3 . 5 4 . 0 4 . 5 5 . 0 5 . 5 Placebo Finasteride Doxazosin Combination p < 0.0001 ; df = 3 Percent with Event Years from Randomization
Cumulative Incidence of AUR 4 . 0 3 . 5 3 . 0 2 . 5 2 . 0 1 . 5 1 . 0 0 . 5 0 . 0 0 . 0 0 . 5 1 . 0 1 . 5 2 . 0 2 . 5 3 . 0 3 . 5 4 . 0 4 . 5 5 . 0 5 . 5 Placebo Finasteride Doxazosin Combination p = 0.0034 ; df = 3 Percent with Event Years from Randomization
Cumulative Incidence of BPH Invasive Therapy 1 0 8 6 4 2 0 0 . 0 0 . 5 1 . 0 1 . 5 2 . 0 2 . 5 3 . 0 3 . 5 4 . 0 4 . 5 5 . 0 5 . 5 Placebo Finasteride Doxazosin Combination p < 0.0001 ; df = 3 Percent with Event Years from Randomization
When is Treatment Required?Urologic Consultation Necessary • Total urinary retention • Partial or complete loss of kidney function • Formation of bladder stones • Bleeding • Severe bothersome symptoms (AUA Symptom Score >19)
Classical TURP“Gold Standard” • Most urologists are well trained in TURP • Most effective therapy • TURP today is “much less invasive” than reports from previous decades
Vanderbilt TUIP Experience • 30 consecutive TUIP • UDS Proved BOO • Single incision • < 30 grams • Mean age=45 years • Mean F/U=31 months • 9% retrograde ejaculation
Treatment Algorithm • Assess prostatic symptoms • Examine prostate for cancer screening • Emperic treatment for 6 weeks using an alpha blocker • Consider finasteride or dutasteride • Refer failures for urologic evaluation including pressure/flow urodynamic testing
CRITICAL POINTS • Growth dependent on Zonal Anatomy • Small Prostates Can be Obstructive • Alpha Blocker Effect Dose Dependent • Finasteride or Dutasteride Requires 6+ month treatment duration • Combination therapy is most effective • Less Invasive Surgical Options are less effective than TURP
Types of Prostatitis • Acute bacterial • Chronic bacterial • Nonbacterial (most common) • Prostatodynea • Largest NIH trial showed antibiotics and α-blockers are not helpful for chronic prostatitis!!!!
Prostate Cancer Facts • Leading solid tumor in men* • Second cause of cancer death in men (lung first)† • 2004: 230,100 new cases with 29,900 deaths • Death rate is declining: peak deaths 41,000 in 1997 • 1 in 6 lifetime probability • Many controversies‡ • To screen or not to screen • How to treat • When to treat *Jemal A, et al. CA Cancer J Clin. 2004;54:8-29. †Stephenson RA. Urol Clin North Am. 2002;29:173-81. ‡Cookson MS. Cancer Control. 2001;8:133-40.
Cancer Detection • The total number of new prostate cancer cases detected in the United States annually is now decreasing from a peak in 1994 • Probably due to the introduction of the PSA assay in the late 1980’s. Many early stage cancers were detected in the early 1990’s that would otherwise not have become evident for many years
Prostate Cancer Mortality: NCI 0 -2 -4 % -6 Change in Mortality -8 1990–1995 Caucasian -10 African American -12 -14 All Ages <65 Years 65+ Years Mettlin CJ, et al. Cancer. 1998;82:249-251.
Evidence for Screening • Fall in mortality now seen • SEER* • Olmsted County, MN† • Canada/Quebec‡ • US Department of Defense (DoD) • Tyrol, Austria • Mortality fall not seen (where PSA screening not or less-commonly performed) • Mexico • Europe SEER=Surveillance, Epidemiology, and End Results *Levy IG. Cancer Prev Control. 1998;2:159; †Roberts RO, et al. J Urol. 1999;161:529-33; ‡ Meyer F, et al. J Urol. 1999;161:1189-91.
Cost Analysis of Screening Cost perIntervention QALY Gained Liver transplantation $237,000 Screening mammography (< age 50) $232,000 Worst case—CaP Screening $145,600 CABG—two vessel/angina $106,000 Captopril for hypertension $ 82,600 Hydrochlorothiazide for hypertension $ 23,500 Best case—CaP Screening $ 8,700 Stop smoking MD message $ 1,300 QALY=quality-adjusted life years; CaP=prostate cancer; CABG=coronary artery bypass graft Thompson IM, Optenberg SA. Oncology (Huntingt). 1995;9:141-5.
Risk in African American Men • Probability of an American black man being diagnosed with CaP and dying from CaP is 85% and 114% greater, respectively, than his fellow white countrymen. • Native Americans, Hispanics and Orientals have a lower risk of dying from prostate cancer than white Americans.
Prostate Cancer Work-up • Annual PSA blood test when >50 age <70 • Digital rectal exam • Biopsy any digital abnormality or elevated PSA • Bone scan not needed if PSA< 15 • CT scans and CXR not helpful for staging • Benefit of other testing methods unclear
Use of Percent Free PSAin 4 – 10 ng/mL Range 60 50 40 Positive 30 Biopsy (%) 20 10 0 <10% 10%–15% 15%–20% 20%–25% >25% Percent Free PSA Catalona WJ, et al. JAMA. 1998;279:1542-1547.
Prostate Cancer Decision Tree • Confined to the prostate (T1–T2) • Surgery, radiation, cryotherapy, observation • Locally advanced (T3–T4) • Surgery, radiation (with or without hormone therapy [HT]), HT • Advanced / Metastatic (N+, M+) • HT (to decrease testosterone levels to slow the cancer) Gomella LG, Fried JJ. The decision tree: the right treatment at the right time. In: Recovering from Prostate Cancer. New York: Harper Collins; 1993. Harris KA, Reese DM. Drugs. 2001;61:2177-92. Lee F, Patel HR. Hosp Med. 2002;63:465-70.
100 80 60 % 40 20 0 2.6–4 4.1–5 5.1–10 >10 PSA (ng/mL) PSA Levels and Organ-Confined Rates at RRP RRP=radical retropubic prostatectomyCatalona WJ, et al. Urol. 2000;55:791-795.
Prostate Cancer Prevention Trial To determine if finasteride vs. placebo taken for 7 years could reduce the prevalence of CAP Presence or absence of histologically proven CAP at 7 years (interim or end-of-study biopsy/7-year biopsy)
PCPT Conclusions • PCPT ended prematurely; objectives met • CAP in 24.4% (1147 of 4692) of placebo and 18.4% of finasteride (803 of 4368) (24.8% reduction) • High grade CAP (Gleason score 7–10) in 237 (5.1%) of placebo and 280 (6.4%) of finasteride; 43 more cases in treatment arm • Some concern over slight increase in high Gleason score in finasteride arm (?? artifact caused by hormonal treatment) • The first clinical trial in which an intervention in healthy men reduced the risk of CAP Thompson IM. N Engl J Med. 2003;349:213-224.
CRITICAL POINTS • Combination of PSA and DRE most sensitive screening (detects about 80%) • Men 70 or under and in good health should be offered curative therapy • No reason to screen men who are not candidates for curative therapy • Watchful waiting is reasonable for men >70