Benign Prostatic Hyperplasia (BPH)
450 likes | 953 Views
Learn about the prostate, BPH, symptoms, complications, and diagnostic tests for men's health. Understand the impact on urination and bladder function due to prostate enlargement. Get insights on management and treatment options.

Benign Prostatic Hyperplasia (BPH)
E N D
Presentation Transcript
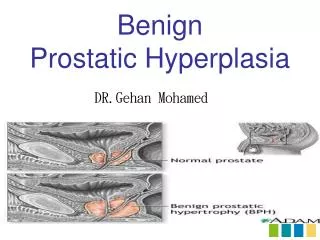
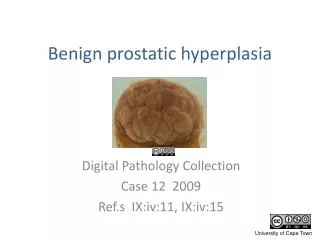
Location and function of the prostate • The prostate is a small gland present only in men which is about the size of a chestnut. • The prostate lies just below the bladder and fits around the urethra rather like a collar. The urethra is the tube through which both urine and semen pass out of the body.
Location and function of the prostate • The prostate produces a fluid which forms a part of the semen. During sexual intercourse, sperm pass from the seminal vesicles into the urethra and are carried through the urethra in fluid squeezed out from the prostate gland during orgasm. • The rest of the semen is stored in the paired seminal vesicles which lie just behind the prostate. • The prostate depends on the testes functioning normally for its normal growth and development.
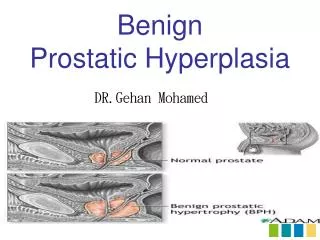
Enlargement of the prostate gland • In many, indeed, most men, the prostate progressively enlarges as they get older. More than 50% of men over the age of 60 and 80% of men over the age of 80 have benign (i.e. not cancerous) enlarged prostates. • Doctors call this enlargement of the prostate 'benign prostatic hyperplasia' or 'BPH' for short.
Enlargement of the prostate gland • As the prostate enlarges, it presses on the urethra, which is the tube that carries the urine and semen out of the body. This causes obstruction, making it difficult to pass urine. It may also make you want to go to the toilet more often and empty the bladder incompletely. Because of the extra work the bladder has to do to overcome this obstruction, its wall becomes thickened and less distensible. • Although some of the obstruction is due to the physical enlargement of the prostate gland, another important element is an increase in the amount of muscular tissue in the prostate. Contraction of this muscle, perhaps brought on by cold or anxiety, may make obstruction worse resulting in even more difficulty with the passage of urine.
Symptoms of prostate enlargement • Because the prostate enlarges very gradually, few changes are noticed at first. However, as the prostate gets bigger and presses on the urethra more, the stream of urine may become weaker or the urine flow only starts after a period of waiting - this is called hesitancy. • Eventually, the enlargement of the prostate may also affect the bladder, causing other symptoms, such as having to go to the toilet more frequently, or having to get up several times during the night. Some men may also experience a need to pass urine urgently, stopping and starting during the stream, dribbling at the end of the stream, and occasional leakage of urine (incontinence).
Symptoms of prostate enlargement • When the prostate becomes very obstructive, it may make it extremely difficult to pass urine or it may block the urethra completely. • Complete blockage of the urethra is serious and requires admission to hospital so that a catheter (a narrow tube) can be passed up the urethra into the bladder to drain off the urine. Subsequently, prostate surgery to relieve the obstruction is usually necessary.
Bladder problems • If an enlarged prostate has been pressing on the urethra for a long time, the back pressure can eventually damage the bladder and also less commonly affect the kidneys. • Bladder stones may form and block the opening of the bladder into the urethra or lead to infection. • Thickening of the bladder wall causes irritability, increasing the frequent need to pass urine.
Bladder problems • Distension of the ureters and back pressure on the kidneys may produce tiredness and loss of appetite. • Because of the high pressures in the bladder, 'pouches' called diverticula may form at weak points in the bladder wall. This may result in the need to pass urine twice in rapid succession.
MANDATORY TESTS History Obtain an adequate medical history by enquiring about: - The urinary tract - Previous surgical procedures (particularly affecting the genitourinary tract) - General health matters - Medications currently taken by the patient - Patient's fitness for possible surgery
Quantification of symptoms Symptoms should be quantified by using the International Prostate Symptom Score (I-PSS) and Quality of Life Assessment, as shown in Figure 6. The scores derived allow this tentative classification of symptoms as shown in Table I.
Physical examination Physical examination should assess: - Suprapubic area to rule out significant bladder tone - Sphincter tone Bulbocavernosus reflex plus brief assessment of motor and sensory function in lower body Digital rectal examination (DRE) This procedure should be performed to evaluate the prostate gland with regard to approximate size, consistency, shape, and abnormalities suggestive of prostate cancer.
Interpreting results of DRE BPH and prostate cancer are two distinct diseases, although they may co-exist in the same patient. Patients should be advised that no clear evidence exists that BPH predisposes to development of cancer. Further, patients should be reassured that, if BPH is diagnosed, prostate cancer is more likely to be detected at an earlier - and more treatable - stage due to the extra vigilance afforded their genitourinary functions. DRE is mandatory when trying to assess any symptomatic bladder-outlet dysfunction; the two conditions usually present quite distinct signs during rectal examination
Urinalysis Urinalysis is performed either using a dipstick test or by examination of urinary sediment following centrifugation. It is used to determine if the patient has - Haematuria - Proteinuria - Pyuria Renal-function assessment - Should be determined by serum creatinine test
RECOMMENDED TESTS Uroflowmetry Uroflowmetry, an non-invasive technique, is recommended in the initial diagnostic assessment and whenever appropriate during and after treatment to determine response . Maximal urinary flow rate (Qmax) is the best single measure, but a low Qmax does not distinguish between obstruction and decreased bladder contractility. Because of great individual variability of flow rate, and the volume dependency of the peak urinary flow rate, at least two uroflow measurements should be obtained, with a resulting volume ideally more than 150ml If such a volume cannot be obtained with repeated uroflowmetries, the Qmax at available voiding volumes should then be taken into consideration.
RECOMMENDED TESTS Residual urine The determination of residual urine is recommended in the initial diagnostic assessment of the patient during and after treatment to determine response. The determination is best performed by noninvasive transabdominal ultrasonography . This will simultaneously provide information about bladder capacity and bladder-wall changes and can detect the presence of bladder stones, diverticula, and a median lobe. The invasive nature of any other means (i.e., catheterisation) of determining residual urine must be weighed against the benefits of the test.
OPTIONAL TEST Prostate specific antigen The clinical distinction between BPH and prostate cancer cannot be accomplished with certainty by DRE and physical examination.PSA determination and DRE in combination provide the best means to determine the pretreatment probability for prostate cancer and, consequently, the need for a prostate biopsy. PSA is an important indicator of prostate cancer because it is a protein secreted exclusively by prostatic epithelial cells and is elevated in the serum of most patients with BPH or prostate cancer. Gram for gram, however, prostate cancer can increase serum PSA as much as 10 times more than BPH.
X-Ray Examination • Excretory urography • Retrograde cystography • Retrograde urethrography gives only indirect information on the effect of benign prostatic enlargement (BPE) on adjacent structures.
Cystoscopy • The standard endoscopic procedure for diagnostic evaluation of the lower urinary tract (urethra, prostate, bladder neck and bladder) is a urethrocystoscopy. • This investigation can confirm causes of outflow obstruction while eliminating intravesical abnormalities.
Treatment of prostate enlargement • Most treatments for prostate enlargement aim to reduce the size of the prostate and its restrictive effect on the urethra. This may be done either with drugs or by surgery. Those with only minor symptoms need no treatment. This is sometimes called 'watchful waiting'. • The 'ideal' treatment is one that is both very effective and has very few side-effects. In reality, those treatments that are most efficient in 'unblocking' the urethra also carry a higher risk of side-effects than treatments which are not so effective.
Treatment of prostate enlargement • In general, if symptoms are mild or moderate, either no treatment or treatment with tablets will be tried at first. The risk of side-effects with tablets is small and they usually disappear if treatment is stopped. • If symptoms are very bothersome and severe, however, surgery is often necessary. This is generally safe and effective, but is likely to reduce the volume of semen produced at the time of orgasm, because the semen passes backwards into the bladder (retrograde ejaculation). • A number of new 'minimally invasive' forms of treatment have recently been developed, such as laser prostatectomy. Although some of these treatments are promising, we do not yet know how effective they are in the longer term.
Alpha blockers • The prostate consists mainly of two types of tissue - glandular tissue and smooth muscle. Alpha blockers are drugs that can 'relax' the smooth muscle of the prostate. This reduces the pressure on the urethra and provides relief from some of the symptoms caused by the enlarged prostate. • Treatment with alpha blockers usually improves symptoms within 2-3 weeks. Altogether, about 60-75% of patients gain some benefit from these drugs.
Alpha blockers • When taking alpha blockers, some patients may experience side-effects, such as headaches, dizziness, lightheadedness (faintness) or tiredness; if you are affected, you may find that these effects often wear off if you keep taking the tablets. Most alpha blockers also lower blood pressure if it is raised; this can be an extra benefit if you suffer from high blood pressure. • Patients who are prone to fainting attacks or have low blood pressure should avoid alpha blockers.
5 alpha reductase inhibitors • 5 alpha-reductase inhibitors block the effect of the male sex hormone, testosterone, on the prostate by preventing formation of the more active hormone dihydrotestosterone (DHT). It is thought that this is the main hormone involved in prostate enlargement. • 5 alpha-reductase inhibitors are drugs that work by reducing the amount of DHT produced. Without this hormone, the prostate will stop getting larger and may, in some cases, shrink. As a result, symptoms will not get any worse and often improve.
5 alpha reductase inhibitors • It may take up to 6 months to get the best improvement in symptoms. If treatment is stopped, the prostate tends to enlarge again. Overall, more than half of all patients treated benefit from these drugs. • In a very few patients (3-5%), 5 alpha-reductase inhibitors can reduce sex drive and erections, but these side-effects are reversible if treatment is stopped.
Transurethral incision of the prostate (TUIP) • Transurethral incision of the prostate (TUIP) is not the most common prostate operation, but may be the most suitable procedure when the prostate is still quite small, and is becoming increasingly popular with urologists. • TUIP is a simple operation, carried out under a general anaesthetic, which only takes about 15 minutes. The procedure involves passing an instrument up the urethra and making one or two small cuts in the bladder neck and prostate. These cuts allow the prostate tissue around the urethra to spring apart. This reduces the pressure of the prostate on the urethra and makes it easier to pass urine.
Transurethral incision of the prostate (TUIP) • During the operation, a catheter will be passed up the urethra into the bladder to drain off the urine. This will be removed after 24 hours. You will usually be able to go home 2-3 days after admission. • Most patients find that symptoms and urine flow improve after the operation. • A few patients (up to 15%) may experience 'retrograde ejaculation' after the operation. This means that the semen pass backwards into the bladder during orgasm instead of out of the penis. It is not harmful and the semen will come out naturally the next time you pass urine. • In the unlikely event that symptoms recur after TUIP, you may need further surgery. This will usually be an operation called transurethral resection of the prostate (TURP).
Transurethral resection of the prostate (TURP) • Transurethral resection of the prostate (TURP) is the most frequently performed operation for prostate enlargement. It is carried out under a general anaesthetic and usually takes about 30-60 minutes. TURP involves passing an instrument up the urethra and cutting away the middle of the enlarged prostate. • During the operation, a catheter will be passed up the urethra into the bladder to drain off the urine. This will be removed after 36-48 hours. You will usually be able to go home after 3-4 days, but will need to 'take life quietly' for a few weeks. • The flow rate usually improves rapidly after the operation, but the need to pass urine frequently may take a few months to subside. Some men complain of an urgent need to void and a burning sensation on passing urine after the operation, but this will usually disappear within a few days or weeks.
Transurethral resection of the prostate (TURP) • Bleeding into the urine for several days or even weeks is normal after TURP, but the urine will gradually clear. If bleeding is particularly heavy and persistent, the urine will be checked to make sure there is no infection. • Many men develop 'retrograde ejaculation' after the operation. This means that the semen pass into the bladder during orgasm instead of out of the penis. This is not harmful and the semen will come out the next time you pass urine. • About 80-90% of patients benefit from TURP, but sometimes , after surgery, the prostate may regrow and cause obstruction again. As a result, about 10% of men will need a second operation within 5 years.
Retropubic prostatectomy (RPP) • Retropubic prostatectomy (RRP) is an operation that is usually performed only if the prostate is very large by means of a cut through the skin. • The procedure is carried out under general anaesthesia and takes about 1 hour to perform. • In open prostatectomy, part of the prostate is removed through a cut made in the lower abdomen, which will leave a scar. • During the operation, a catheter will be passed up the urethra into the bladder to drain off the urine. This will be removed after 3-4 days. You will be able to go home after about 1 week.
Retropubic prostatectomy (RPP) • Most patients experience an immediate improvement in urine flow, but the need to pass urine frequently may persist for some weeks or even months. • A period of convalescence of 4-6 weeks is advisable, because of weakness and tiredness after the operation. • The pieces of the prostate removed during surgery are examined under the microscope to make sure there are no tiny areas of prostate cancer present. • Because not all the prostate tissue is removed, men who have this operation remain at some risk of developing prostate cancer.
Prostatic stents • Unlike most treatments for prostate enlargement, stents overcome the narrowing of the urethra caused by the enlarged prostate, rather than by reducing the size of the prostate itself. Stents are small metal coils that are inserted into the urethra to hold the walls open. • Two types of stent are available - temporary and permanent. • The insertion of these devices is carried out under light, general anaesthesia and takes less than 15 minutes.
Prostatic stents • The stent is placed within the prostate with the help of a telescope. After the operation, passing urine may be uncomfortable for some weeks. • Stents do have some disadvantages. Both permanent and temporary stents can become encrusted with calcium salts. The presence of a stent also increases the risk of urinary tract infection (cystitis). Temporary stents can also 'slip' from their position in the urethra and have to be replaced every 6 months. With permanent stents, the tissue'of the urethra may grow through the holes in the mesh of the coil and cause obstruction again.
Transrectal hyperthermia • Transrectal hyperthermia uses microwave energy to destroy some of the prostate tissue by heat. • The procedure is carried out without anaesthesia and takes about 60 minutes; up to six treatments are usually necessary. • A probe is inserted into the back passage (rectum) and directed towards the prostate. The prostate tissue is then heated to about 41-45°C; a cooling system ensures that heat from the probe does not damage other tissues.
Transrectal hyperthermia • The procedure is usually carried out on a day-case basis and seldom has significant side-effects other than mild rectal discomfort and burning on passing urine. • Transrectal hyperthermia may improve symptoms in some men, but it is a new technique that is still under investigation and many urologists doubt its long-term effectiveness.
Transurethral thermotherapy • Transurethral thermotherapy uses microwave energy to destroy some of the prostate tissue by heat. • The procedure is carried out under local anaesthesia, which means that you will be awake throughout the operation, which takes about 60 minutes. Occasionally, some sedation is needed. • A catheter containing a microwave coil is inserted into the urethra. The prostate tissue is then heated to about 45-55°C. A cooling system ensures that heat from the coil does not damage other tissues and the temperature of other tissues is monitored using a device that is inserted into the back passage (rectum). The damaged prostate swells initially, but then shrinks.
Transurethral thermotherapy • Immediately after the operation, you may find it difficult to pass urine and may experience a burning sensation. • Transurethral thermotherapy improves symptoms in some men, but it is a new technique, which is still being assessed and improved. One disadvantage of the technique is that up to 25% of patients experience temporary urine retention (an inability to pass urine) afterwards, because of swelling. The long-term results are probably not as good as conventional surgery.
Laser therapy • Laser energy is used to destroy some of the prostate tissue by intense local heat. The procedure is carried out under a general anaesthetic and takes about 20 minutes. • A laser probe is inserted through the urethra and the prostate tissue is then treated with the laser. Some of the tissue that is destroyed is removed during the operation, but most is washed away afterwards in the urine over a number of months. • Bleeding after laser therapy is rare, but the treated area will feel sore and you will feel a burning sensation when you pass urine for 4 weeks or longer. Urinary infections may also occur. • After the operation, a catheter will be passed up the urethra into the bladder to drain off the urine. This will be removed after a few days. You will be able to go home after 1-2 days, but may need a catheter for rather longer.
Laser therapy • About 30% of men suffer 'retrograde ejaculation' after the operation. This means that the sperm pass into the bladder during orgasm instead of out of the penis. Impotence is uncommon and both problems are rather less common than after conventional prostate surgery. • As the prostate tissue is destroyed during the operation, it cannot be examined under the microscope to make sure there is no cancer present. However, your doctor would not use this technique if he thought that there was any chance of prostate cancer. • This is a new procedure and the long-term effectiveness of this form of treatment is not yet known.
High intensity focused ultrasound therapy • High intensity focused ultrasound is a very new technique that is used to destroy some of the prostate tissue by heat. • The procedure is carried out under general anaesthesia and takes about 30 minutes. • An ultrasound probe is inserted into the back passage (rectum) and directed forwards towards the prostate to destroy the tissue. The damaged tissue shrinks with time, producing an improvement in symptoms and urinary flow.
High intensity focused ultrasound therapy • There is minimal discomfort afterwards, but there may be some difficulty passing urine and a catheter is often necessary for a few days. • An advantage of this technique is that it causes little or no bleeding, and few side-effects. • As the prostate tissue is destroyed during the operation, it cannot be examined under the microscope to make sure there is no cancer present. • This is a new procedure and the long-term effectiveness of this form of treatment is not yet known.