Download
1 / 112
1.12k likes | 1.15k Views
Learn to classify, diagnose, and treat central nervous system infections. Understand the etiologic agents, symptoms, and prognosis of CNS infections like meningitis and encephalitis. Enhance your knowledge of the clinical presentation and complications of acute CNS infections.

E N D
CENTRAL NERVOUS SYSTEM INFECTIONS Dr. Meral SÖNMEZOĞLU InfectousDiseasesDepartment YEDİTEPE UNIVERSITY HOSPITAL
Learningobjectives • Classify central nervous system infections • Understand the pathophysiology of central nervous system infections • Know the possible etiologic agents at certain ages • Know the symptoms, signs and diagnosis of central nervous system infections • Know treatment modalities of central nervous system infections • Understand prognosis and know complications • Be alert to the clinical presentation of acute central nervous system infections
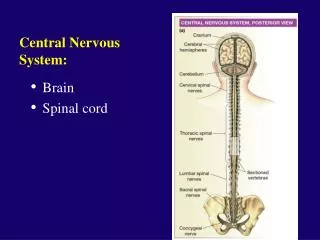
CNS Infections • Meningitis • Bacterial, viral, fungal, chemical, carcinomatous • Encephalitis • Bacterial, viral • Meningoencephalitis • Abscess • Parenchymal, subdural, epidural
CNS Infections • Signs and symptoms • Fever • Headache • Altered mental status -lethargy to coma • Neck stiffness – meningismus – flex/ext • Increased intracranial pressure – papilledema, nausea/vomiting, abducens palsies, bulging fontanelle in infants
Meningitis • Bacterial • Viral ( aseptic) • TB • Fungal • Chemical • Parasitic • ? Carcinomatous
Classification of Meningitis • Infectious • Bacterial • Viral • Fungal • Non-infectious • Drug-Induced • Neoplastic • Autoimmune
Noninfectious.. Metabolic Mitochondrial (Reye’s, MELAS) NMS (Neuroleptic malignant syndrome) Nutritional deficiency (Wernicke’s) Paraneoplastic PRES or Malignant hypertension Seizures – (non-convulsive status) TBI Toxic Vascular
BacterialMeningitis • Definition • Bacterial meningitis is an inflammatory response to bacterial infection of the pia-arachnoid and CSF of the subarachnoid space • Epidemiology • Incidence is between 3-5 per 100,000 • More than 2,000 deaths annually in the U.S. • Relative frequency of bacterial species varies with age.
Routes of Entry • Hematogenous • Neighboring focus • Anatomic defect • congenital • traumatic • surgical • Intraneural pathways
Bacterial Meningitis • Streptococcus pneumoniae • Hemophilus influenzae • Listeria moncytogenes • Group B streptococcus • Niesseria meningitidis
NeonatalMeningitis Bacteria are often acquired from the maternal vaginal flora. Gram-negative enteric flora and GBS are the dominant pathogens. L monocytogenes is another well-known but fairly uncommon causative pathogen.
NeonatalMeningitis Early-onset GBS meningitis occurs during the first 7 days of life as a consequence of maternal colonization and the absence of protective antibody in the neonate. Pathogens are acquired before or during the birth process. Late-onset meningitis is defined as disease occurring after 7 days of life. Causes include perinatally acquired and nosocomial pathogens. Streptococcus agalactiae(GBS) serotype III causes 90% of late-onset disease. Underdeveloped countries, gram-negative bacilli—specifically, Klebsiella organisms and E coli —may be more common than GBS.
Children In children older than 4 weeks: S pneumoniae and N meningitidis are the most common etiologic agents. Hib has essentially disappeared in countries where the conjugate vaccine is routinely used.
Streptococcus pneumoniae the predominant cause of bacterial meningitis (58.0% of cases), • group B streptococcus (GBS) (18.1%) • Neisseria meningitidis (13.9%), • Haemophilus influenzae (6.7%), • Listeria monocytogenes (3.4%).
Meningitis • Pathogenesis • Majority of cases are hematogenous in origin • Organisms have virulence factors that allow bypassing of normal defenses • Proteases • Polysaccharidases
Meningitis • Pathology and Pathogenesis • Sequential steps allow the pathogen into the CSF • Nasopharyngeal colonization • Nasopharyngeal epithelial cell invasion • Bloodstream invasion • Bacteremia with intravascular survival • Crossing of the BBB and entry into the CSF • Survival and replication in the subarachnoid space
Interrupted arrows indicate where a diffusion of water or solutes can occur between brain capillaries, CSF, and nervous tissue: (a) across the blood-brain barrier; (b) across the epithelium of the choroid plexus; (c) across the ependyma; (d) across the pia-glial membranes at the surface of the brain and spinal cord; (e and f) across the cell membranes of neurons and glial cells. The thick line represents the dura mater and arachnoidea surrounding the system
Pathophysiology of Bacterial Meningitis • Bacterial colonization within the subarachnoid space • Initiation of inflammatory response which leads to: • Endothelial damage • Disruption of the blood-brain barrier • On a larger scale, this results in: • Cerebral edema • Cytotoxic • Vasogenic • Interstitial • Increased ICP
Pathophysiology of Bacterial Meningitis • Pathology • Hallmark • Exudate in the subarachnoid space • Accumulation of exudate in the dependent areas of the brain • Large numbers of PMN’s • Within 2-3 days inflammation in the walls of the small and medium-sized blood vessels • Blockage of normal CSF pathways and blockage of the normal absorption may lead to obstructive hydrocephalus
Pathophysiology of Bacterial Meningitis Complications: • Seizures • Hydrocephalus • Infarction • Herniation From van de Beek D Community-acquired bacterial meningitis in adults. 354:1. 44.
ClinicalPresentation of Meningitis • Classicsigns ; • fever, headache, neckstiffness, photophobia, nausea, vomiting, andsigns of cerebraldysfunction (eg, lethargy, confusion, decreased level of consciousness coma). • Thetriad of fever, nuchalrigidity, andchange in mentalstatus is found in onlytwothirds of patients • Atypicalpresentationmay be observed in certaingroups (elderly, diabetic, neutropenic, immunocompromisedhosts..).
ClinicalPresentation of Meningitis • Signs of cerebral dysfunction are common, including confusion, irritability, delirium, and coma. These are usually accompanied by fever and photophobia. • Signs of meningeal irritation are observed in only approximately 50% of patients with bacterial meningitis, and their absence certainly does not rule out meningitis
Meningitis • Clinical Manifestations – Nuchal rigidity • Kernig’s • Pt supine with flexed knee has increased pain with passive extension of the same leg • Brudzinski’s • Supine pt with neck flexed will raise knees to take pressure off of the meninges • Present in 50% of acute bacterial meningitis cases • Cranial Nerve Palsies • IV, VI, VII • Seizures
Amos’s Sign Hips & knees flexed Back arched Neck in extension Trunk supported by arms
Meningitis • Focal neurologic signs may develop as a result of ischemia from vascular inflammation and thrombosis • Papilledema and other signs of increased ICP may be present. • Coma, increased blood pressure with bradycardia, and cranial nerve III palsy may be present. • The presence of papilledema also suggests a possible alternate diagnosis (eg, brain abscess).
Meningitis Papilledema
Exam in suspected CNS Infection • Mental Status • Cranial nerve and fundiscopic exam • Meningeal Signs • General exam – rashes, lymphadenpathy • Labs – CBCD, BMP, PT/PTT, bHCG, blood cultures, UA C&S • Radiology – CT head - uncontrasted if no focal signs, contrast if mass suspected
Key CSF Features • CSF is not liquid gold – get enough to get your answer • CSF Glucose is 2/3 of serum glucose • Important in diabetic patients • Traumatic LPs – • CSF pro increases by 1 for every 1000 rbcs • Tube #1 and Tube#4 for rbcs when SAH is in the differential not as a routine • Very high CSF Protein levels will make CSF yellow • Send a full tube of CSF for cytology not just a few cc’s
Diagnosis of Meningitis • Diagnosis • Assess for increased ICP • Papilledema • Focal neurologic findings • Defer LP until CT scan or MRI obtained if any of above present • If suspect meningitis and awaiting neuroimaging • Obtain BC’s and start empiric Abx
Diagnosis of Meningitis Obtain CT scan before lumbar puncture in patients with: • Immunucompromised state • History of CNS disease • New onset seizures • Papilledema • Altered level of consciousness • Focal neurologic signs
Diagnosis of Meningitis • Obtain blood cultures and give empiric antibiotics if LP is delayed
LP Increased intracranial pressure is expected – but LP contraindicated if a mass is present or if epidural spinal abscess is suspected Left lateral decubitus position L3-L4 interspace or L4-L5 interspace Think about your studies before the LP