Download
1 / 32
320 likes | 536 Views
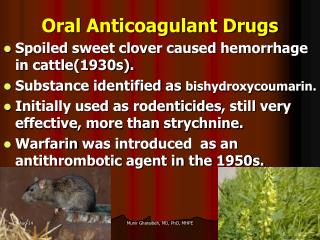
Angioplastie coronaire et traitement anticoagulant oral. Dr. Joseph Elias. Indications d’anticoagulation orale. Fibrillation auriculaire Maladie thomboembolique AVC EP Valves mécaniques. Autre indications cardiaques Thrombus VG Anévrysme ventriculaire Altération de la fonction VG

E N D
Angioplastie coronaire ettraitementanticoagulant oral Dr. Joseph Elias
Indications d’anticoagulation orale • Fibrillation auriculaire • Maladie thomboembolique • AVC • EP • Valves mécaniques • Autre indications cardiaques • Thrombus VG • Anévrysme ventriculaire • Altération de la fonction VG • Indications non cardiaques • Déficit en proteine S
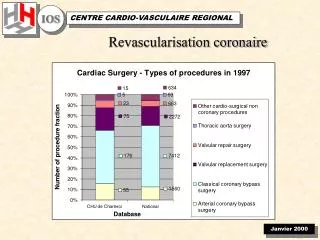
ATC et AVK • 120000 angioplasties par an en France • 3 a 4% réalisées sous anticogulants • 3600 patients par an necessitent l utilisation de deux antiagrégants associés ou non a des anticoagulants
Données de laLitterature • Registres retrospectifs ++ • Recommandations internationales??? • Etudes randomisées !!!
AA+Aspirine: 1.6% AVK + Aspirine: 6.2% Randomisation AA+Aspirine et AVK+Aspirine après stenting chez 517 pts Schomig et al NEJM 1996;334:1084-9
ISAR, STARS, FANTASTIC, MATTIS % MACE à 30 jours avec AVK et Aspirine X 2 1653pts 496pts 485pts 350pts STARS NEJM 1998, 339:2126-32 ISAR Circulation 1997,96:462-7 FANTASTIC Circulation 1998;98:1597 MATTIS Circulation 1998;98:2126-32
% de saignements sous AVK et aspirine 1653pts 496pts 485pts 350pts STARS NEJM 1998, 339:2126-32 ISAR Circulation 1997,96:462-7 FANTASTIC Circulation 1998;98:1597 MATTIS Circulation 1998;98:2126-32
Clopidogrel VS Ticlopidine • A 30 jours As + Clopidogrel: MACE = 2% Métaanalyse de Bhatt et al JACC 2002;39:9-14
Incidence de thromboses et saignements en fonction de l’INR 530 pts avec ATC (34% stent) et AVK + As % Accidents thrombotiques ou hémorragiques est le plus bas 2.5 <INR <4 Accidents thrombotiques Accidents hémorragiques INR >4 Berg et al Circulation 2001;103:2042-47
Registre de la Mayo Clinic Saignements: 30 J 9.3% 2 majeurs DC=0 Thrombose stent=0 % 66 pts ayant un stent et As + Clopidogrel + AVK Orford et al Am Heart J 2004;147:463-7
Registre Rubboli 55%: 3 TT MACE à 30 jours: 18% 27 pts sous AVK au moment de l’ATC Etude rétrospective Rubboli et al Ital Heart J 2004;5:919-25
Registre Porter 180 pts sous AVK durant 1 mois en post ATC Etude retrospective à 12 mois +++ 57.8% (104 pts) poursuivent le TTT par AVK et aspirine pendant 376 days Porter et al Cath Cardio Intervention 2006;68:56-61
Registre Porter 180 pts sous AVK durant 1 mois en post ATC Etude retrospective à 12 mois • Saignements: 20 (11%) • Majeurs: 2 hématomes du scarpa • Mineurs: 18 • 18 /20 surviennent au cours de la jonction entre AVK et héparine post PCI Porter et al Cath Cardio Intervention 2006;68:56-61
Registre GRACE Facteurs prédictifs OR Age>80 1.82 Femmes 1.65 Creatinine > 2mg/dl 2.06 ATCD de saignements 2.28 ATC 2.36 Quelle que soit la présentation clinique le risque de saignement augmente le risque de décès hospitalier Moscucci et al EHJ 2003;24:1815-23
En l absence de recommandation officielle concernant la CAT chez les patients ayant une indication formelle des AVK. Quel est le TTT optimal après mise en place d’un stent chez ces patients ????
Stratification du risque thrombotique Patients à haut risque • Risque annuel d’AVC sous AVK Rothberg et al Ann Intern Med. 2005; 143:241-250
Stratification du risque thrombotique • Patients sous AVK: • Risque élevé d’événements thrombotiques • FA et score de CHADS ≥ 2 • Valves mécaniques • Thrombus VG • ATCD de maladie thromboembolique • Risque faible à moderé d’événements thrombotiques • AC/FA (CHADS2 < 2) • CMD
thrombose Saignement STENTICO STENT et antICOagulants
STENTICO • Registre national prospectif multicentrique • Prise en charge des pts sous AVK devant avoir une ATC avec stent • FU à 2 mois et 1 an De Juin 2005 à Novembre 2006 35 centres
STENTICO 400 pts en 17 mois % Age: 72 ± 9 Sex: 82% M Diab: 30% ATCD ATC 25% Pont 12% IDM 28% CHADS2≥2: 52%
STENTICO % 2 Groupes: Triple association: 148 pts Clop et ASA: 252 pts
STENTICO Triple TTT Clopi+Asp N 135 230 Age: 72 +/- 9 71 +/- 9 Sex M : 80% 82% CHADS2 ≥ 2: 54% 54% %
STENTICO % TTT Clopi+A DC: 2 0 MACE: 1 2 Saignements 8 18 AVC: 0 0 • Complications hospitalières
STENTICO Triple TTT Clopi+ASA DC CV 1 1 DC non CV 3 3 MACE : 4 6 Saign: 8 12 AVC: 0 1 FU2 mois : 80% %
STENTICO Ces donées sont préliminaires et méritent une analyse détaillée en fonction du risque thromboembolique initial Importance du suivi +++ Résultats : novembre 2007
CONCLUSION En l absence de recommandations internationales et devant les faibles renseignements que nous apporte la litterature internationale on vous propose une CONDUITE PRATIQUE basée sur une stratification des risques ischemiques et ou hemorragiques qui nous permet de differencier deux groupes et deux attitudes :
Patients a haut risque (FA avec CHADS>2,valve mecanique,thrombus mural,maladie thromboembolique preexistante) • Poursuivre les anticoagulants • Traitement avant angioplastie par clopidogrel • Aspirine IV juste avant l angioplastie • Aspirine +Clopidogrel+anticoagulant pendant un mois • Eviter les anti _GP 2b\3a • Préférer les stents nus
Patients a risque bas et intermediaire FA avec CHADS <2, cardiomyopathie sans phenomene thromboembolique associé • Arrêter les anticoagulants oraux • Heparine de bas poids moleculaire • Pretraitement par aspirine+clopidogrel • Utilisation des anti –GP2b\3apossible • HBPM 3 semaines+Aspirine+clopidogrel • Arrêter le clopidogrel et introduction AVK+aspirine • Arrêter l HBPM quand l INR est correct