Download
1 / 52
530 likes | 697 Views
Clearing the Smoke: Realities & Myths about the Tobacco Epidemic. Clifford E. Douglas, J.D. Director, University of Michigan Tobacco Research Network Lecturer, University of Michigan School of Public Health. Student National Pharmacy Association Webinar February 25, 2014. Topics.

E N D
Clearing the Smoke: Realities & Myths about the Tobacco Epidemic Clifford E. Douglas, J.D. Director, University of Michigan Tobacco Research Network Lecturer, University of Michigan School of Public Health Student National Pharmacy Association Webinar February 25, 2014
Topics • Part I. The persistent epidemic • Part II. Who is harmed? • Part III. Our response
Key Resources from HHS/SG/CDC • http://www.SurgeonGeneral.gov– Surgeon General Reports, executive summaries, fact sheets, consumer guides • http://www.cdc.gov/tobacco - statistics, reports, plain language products for download and ordering • http://www.BeTobaccoFree.gov - information portal for additional tobacco-related websites • http://www.smokefree.gov - help for people who want to quit smoking • http://www.cdc.gov/tips - stories of real people dealing with smoking-related diseases and how they quit
Part I. The Persistent Epidemic
The Health Consequences of Smoking:50 Years of Progress 1964 2014
An Amazing Public Health Achievement • In the last half century, lower smoking rates have saved about 8 million lives in the U.S. Average life expectancy has increased by about 10 years, almost a third of which – about 3 years – is due to reductions in tobacco use Source: Theodore R. Holford, et al., Tobacco Control and the Reduction in Smoking-Related Premature Deaths in the United States, 1964-2012, JAMA 2014;311:164-171.
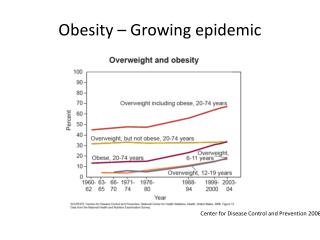
Then… Now… 2013: 18% 1965: 43%
Myth: The Tobacco Problem is “Solved” • 42 million adults and 3 million middle & high school students are smokers • Tobacco causes 480,000deaths per year • Annual costs: $132 billion in medical expenses, $157 billion in lost productivity
Smoking Remains #1 Cause of Preventable Death & Disease • Since 1964, cigarette smoking has killed more than 20 million Americans, including: • 2.5 million nonsmokers • More than 100,000 babies
Smoking Still Kills More Americansthan All of these Combined AIDS Alcohol Car crashes Fires Cocaine Heroin Suicide Homicide
“Most of the tobacco epidemic remains in the future.” Robert Proctor, Ph.D., Stanford University Historian of Science, author of Golden Holocaust: Origins of the Cigarette Catastrophe and the Case for Abolition (2011) 20th Century: 100 million deaths 21st Century: 1 billion deaths (projected)
“The Dirty Dozen” (of 70 carcinogens) Acetone(solvent and paint stripper) Ammonia(poisonous gas and toilet bowl cleaner) Arsenic(potent ant poison) Benzene(poisonous toxin) Butane(flammable chemical in lighter fluid) Cadmium(carcinogenic chemical in batteries; lung & intestinal irritant) Carbon monoxide (poisonous gas in auto exhaust) Formaldehyde(dead frogs love it) Hydrogen cyanide (deadly ingredient in rat poison) Methanol(jet engine and rocket fuel) Polonium-210(radioactive element and spy-killer) Toluene(poisonous industrial solvent)
Nicotine = The Vector • Cigarettes and other forms of tobacco are addicting. • Nicotine is the drug in tobacco that causes addiction. • The pharmacologic and behavioral processes that determine tobacco addiction are similar to those that determine addiction to drugs such as heroin and cocaine.
2014 SGR Confirms:Nicotine Fuels the Epidemic • BIG TOBACCO MANIPULATES SMOKERS: Congress, FDA and federal courts found: The major U.S. cigarette companies “have designed their cigarettes to precisely control nicotine delivery levels and provide doses of nicotine sufficient to create and sustain addiction while also concealing much of their nicotine-related research. • WANT TO HAVE A BABY? Nicotine “activates biologic pathways … relevant to fetal growth and development, immune function, the cardiovascular system, the central nervous system, and carcinogenesis,” and fetal nicotine exposure “has lasting adverse consequences for brain development” and “contributes to … preterm birth and stillbirth”
Addiction vs. Cessation • 70% of smokers want to quit • Each year, 40% attempt to quit • Each year, 2.5% succeed 2014 SGR: “Tobacco industry advertising and promotional activities cause youth and young adults to start smoking, and nicotine addiction keeps people smoking past those ages.”
James Morgan, President, Philip Morris USA, Testimony Under Oath (April 14, 1997) Q. Do you believe that cigarette smoking is addictive? A. Pharmacologically, my answer is no. If they are behaviorally addictive or habit forming, they are much more like caffeine, or in my case, Gummy Bears. I love Gummy Bears ... and I want Gummy Bears, and I like Gummy Bears, and I eat Gummy Bears, and I don't like it when I don't eat my Gummy Bears, but I'm certainly not addicted to them.
“The primary incentive to cigarette smoking is the immediate salutory effect of inhaled smoke upon bodily function … The physiological effect serves as the primary incentive; all other incentives are secondary. …
“Without nicotine … there would be no smoking. … No one has ever become a cigarette smoker by smoking cigarettes without nicotine. … The physiological response to nicotine can readily be elicited by cigarettes delivering in the range of 1 mg. of nicotine. …
“The cigarette should be conceived not as a product but as a package. The product is nicotine. The cigarette is but one of many package layers. …
“Think of the cigarette pack as a storage container for a day’s supply of nicotine. …
“Think of the cigarette as a dispenser for a dose unit of nicotine. …
“Think of a puff of smoke as the vehicle of nicotine. …
“Smoke is beyond question the most optimized vehicle of nicotine and the cigarette the most optimized dispenser of smoke.”William L. Dunn, Ph.D., chief of the Behavioral Research Group at Philip Morris, “Motives and Incentives in Cigarette Smoking,” paper presented at secret tobacco industry conference sponsored by Council for Tobacco Research on St. Martin, N.A., 1972.
“Nicotine is addictive. We are … in the business of selling nicotine, an addictive drug effective in the relief of stress mechanisms.”Brown & Williamson general counsel Addison Yeaman in an internal memorandum, July 17, 1963
“In a sense, the tobacco industry may be thought of as being a specialized, highly ritualized, and stylized segment of the pharmaceutical industry.”Claude Teague, R.J. Reynolds Tobacco Co., “Research Planning Memorandum on the Nature of the Tobacco Business and the Central Role of Nicotine Therein,” April 14, 1972.
Evade Smoke-Free Laws Discourage Quitting
E-Cigarettes’ Impact on Public Health • Key issue is not e-cigs’ level of harmfulness compared to conventional cigs, but net risk they pose for public health • Promotion of e-cigarettes encourages dual use and ongoing addiction, impeding cessation for some smokers who might otherwise quit • E-cigarette use prompts confusion regarding smoke-free policies • Permitting e-cigarette use where smoking is not allowed is confusing and implies acceptance of addiction • to unregulated nicotine delivery products
Part II. Who is Harmed?
Three Populations Smoke at Highest Rates • The poor (>8 million smokers below poverty level) • The least educated (>22 million smokers with a high school education, or less) • Those with co-morbid mental health or addictive disorders (as many as half of all regular smokers)
Disproportionate Impact onAfrican Americans • 47,000 African Americans die each year from smoking-related diseases • Adult African American smoking prevalence rates are comparable to whites, but African Americans have higher lung cancer rates • 72 percent of African Americans are exposed to secondhand smoke • African Americans are more likely to die from the three leading causes of smoking-related death • Coronary heart disease • Stroke • Lung Cancer • African American men are at least 50 percent more likely to develop lung cancer than white men
College Students = Key Industry Target • 24.8% of full-time college students aged 18-22 years old were current smokers in 2010 • The number of smokers who initiated smoking after age 18 increased from 600,000 in 2002 to 1 million in 2010 • Progression from occasional to daily smoking almost always occurs by age 26 Tobacco companies have carefully studied the attitudes and behaviors of young people, particularly as they go through life transitions, such as attending college.
College Students = Future Casualties • Based on current rates, it is predicted that more than 1 million current college students will die prematurely from tobacco use “If young people don’t start using tobacco by age 26, they almost certainly will never start.” - Surgeon General Regina Benjamin
Part III. Our Response
Advocacy Works “If you think you’re too small to be effective, you have never been in bed with a mosquito.”
To combat the tobacco epidemic, we use several evidence-based policy tools
Smoke-Free Policies • Schools, workplaces, restaurants and bars, parks, playgrounds, beaches, other public places • Protect everyone from secondhand smoke • Improve health of workers and patrons • Prompt more smokers to try to quit • Increase the number of successful quit attempts • Reduce the number of cigarettes that smokers consume • Discourage kids from starting
Tobacco-Free College Campus Initiative Vision: Widespread expansion of tobacco-free policies to institutions of higher learning across the U.S. Please visit http://tobaccofreecampus.org! Goals: Foster a collaborative, cooperative effort among academic institutions and community public health partners Expand awareness in academia and among the public of the need for and benefits of such policies Facilitate information flow and access to technical assistance
Significant Progress • 1,182 campuses in U.S. are now 100% smoke-free indoors and outdoors, with no exemptions, including residential housing facilities (a 52.7% increase since September 2012) • Of those, 811 (two-thirds!) have a 100% tobacco-free policy • Some of the large campuses that have gone completely tobacco-free: • University of California (all 10 campuses) • City University of New York (all 24 campuses) • Arizona State University • University of Oregon • University of Oklahoma • University of Kentucky • University of South Carolina • Montana State University • University of Florida (“Gators don’t chew. They chomp!”) • Emory University Source: Americans for Nonsmokers’ Rights Foundation, http://www.no-smoke.org/pdf/smokefreecollegesuniversities.pdf
FDA Regulation of Tobacco Family Smoking Prevention and Tobacco Control Act, enacted June 2009 FDA regulation of tobacco products and tobacco marketing is necessary to control industry behavior and protect public health
New Law Enacted to Fill a Gap Before June 2009, tobacco products were not regulated for health • No product control • A new ingredient could simply be added to the product without testing or disclosure • No ingredient review or disclosure • Poor consumer information • Cigarette toxins not reported to consumers in any meaningful way
FDA Authority • Applies to cigarettes, smokeless tobacco products and roll-your-own tobacco, and authorizes FDA to deem other tobacco products (e-cigarettes, cigars, pipe tobacco, hookah/shisha, dissolvables, etc.) subject to its jurisdiction • Restricts marketing that appeals to kids, misleads adults or deceptively encourages tobacco use, and strengthens restrictions on sales to youth • Authorizes FDA to regulate the contents of tobacco products and the smoke they emit in order to protect public health • FDA can reduce nicotine to non-addictive levels … if and when it tries, the tobacco industry will go to war • FDA is expected to take action on e-cigarettes
Counter-Marketing http://www.fda.gov/AboutFDA/CentersOffices/OfficeofMedicalProductsandTobacco/AbouttheCenterforTobaccoProducts/PublicEducationCampaigns/TheRealCostCampaign/ucm384433.htm
Tobacco Excise Tax Increases • A 10% increase in price results in: • 7% decline in youth prevalence • 2% decline in adult prevalence • 4% decline in overall consumption
Source: Tax Burden on Tobacco, 2010, and author’s calculations
Other Actions Also Drive Social Norm Change and Help Smokers Quit • February 5, 2014 • “Today, we’ve announced that we are ending the sales of tobacco in all 7,600 CVS/pharmacy stores by October 1. As a health care company, it’s time for us to take a stand and to put our customers, colleagues and patients on a path to better health. Share this if you stand with us in our commitment to go tobacco-free. Learn more: http://bit.ly/1lAcT0Y”