Download
1 / 17
170 likes | 478 Views
Apical Rocking and cardiomyopathy. Current attempts of improving patient selection in cardiac resynchronization therapy (CRT) are mainly based on echocardiographic timing of myocardial velocity peaks . Regional myocardial function is neglected . Apical transverse

E N D
Currentattempts of improving patient selection in cardiacresynchronizationtherapy (CRT) are mainlybased on echocardiographic timing of myocardialvelocitypeaks. Regionalmyocardialfunctionisneglected. Apical transverse motion (ATM) is a new parameter to quantify apical rocking as an integrativesurrogate of both temporal and functional inhomogeneitieswithin the leftventricle. In thisstudy, wetested the predictive value of apical rocking for response to CRT. Methods and results Sixty-nine patients eligible for CRT wereassessed by echocardiographybefore and 11+5 monthsafter pacemaker implantation. Responsewasdefined as leftventricular (LV) end-systolic volume decrease .15%. Rockingwasquantified (ATM) and visuallyassessed by four blindedreaders. Predictive value for CRT response of bothassessments wascomparedwithconventionaldyssynchronyparameters. ATM in the four-chamberview plane differentiated best betweenresponders and non-responders (2.2+1.5 vs. 0.06+1.9 mm, P , 0.0001). Quantified ATM predicted reverse remodellingwith a sensitivity, specificity, and accuracy of 75, 96, and 83% whereasvisualrockingassessment resulted in 89, 75, and 83%, respectively. The accuracy of conventionalparameterswassignificantlylower. Conclusion Apical rockingis a new marker to assess LV dyssynchrony and predict CRT response. It issuperior to conventional parameters. Evenits simple visualassessmentmaybesufficientlyaccurate in the clinical setting. - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
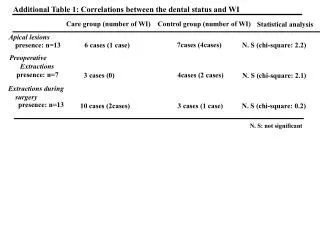
A cut-off of 1.5 mm distinguishedbetweenresponders and nonresponders with a sensitivity, specificity, and accuracy of 75, 96, and 83%, respectively (Figure 2A).
Contradicting reports have been publishedregarding the relation between a dobutamine-inducedincrease in either cardiacdyssynchrony or left-ventricularejection fraction (LVEF) and the response to cardiacresynchronization therapy (CRT). Using apical rocking (ApRock) as surrogatedyssynchronyparameter, weinvestigated the dobutamine stress echocardiography (DSE)-induced changes in left-ventricular (LV) dyssynchrony and LVEF and theirpotential pathophysiologicalinterdependence. Methods and results Fifty-eight guideline-selected CRT candidates wereprospectivelyenrolled for low-dose DSE. Dyssynchronywasquantified by the amplitude of ApRock. An LVEF increaseduring stress of .5% wasregardedsignificant. Scarburdenwas assessed by magneticresonanceimaging. Meanfollow-up after CRT implantation was 41+13 months for the occurrence of cardiacdeath. ApRockduring DSE predicted CRT response (AUC 0.88, 95% CI 0.77–0.99, P , 0.001) and correlated inverselywith changes in EF (r 1/4 20.6, P , 0.001). Left-ventricularejection fraction changes duringDSEwere not associatedwith CRT response (P 1/4 0.082). Linearregressionanalysisrevealed an inverse association of LVEF changes during DSE withboth, total scarburden (B 1/4 22.67, 95CI 23.77 to 21.56, P , 0.001) and the DSE-induced change in ApRock amplitude (B 1/4 21.23, 95% CI 21.53 to 20.94, P , 0.001). Kaplan–Meier analysisrevealedthatDSEinduced increase in ApRock, but not LVEF, wasassociatedwithimproved long-termsurvival. Conclusion Duringlow-dose DSE in CRT candidates withbaselinedyssynchrony, myocardial contractile reservepredominantly results in more dyssynchrony, but less in an increase in LVEF. Dyssynchronyatbaseline and itsdobutamine-induced changes are predictive of bothresponse and long-termsurvivalfollowing CRT.
Currentimaging techniques attempt to identifyresponders to cardiacresynchronizationtherapy (CRT). However, because CRT responsemaydependuponseveralfactors, itmaybeclinically more useful to identify patients for whom CRT would not bebeneficialevenunder optimal conditions. Weaimed to determine the negativepredictive value of a composite echocardiographic index evaluating atrial-ventriculardyssynchrony (AV-DYS) and intraventricular dyssynchrony. Methods and results Subjectswith standard indications for CRT underwentechobefore and during the monthfollowingdevice implantation. AV-DYS wasdefined as a percentage of leftventricular (LV) filling time over the cardiac cycle. AV-DYS, which produces a characteristicrocking of the LV apex, wasquantified as the percentage of the cardiac cycle over which tissue Doppler-deriveddisplacementcurves of the septal and lateralwallsshowed discordance. CRT responder statuswasdeterminedbased on the earlyhaemodynamicresponse to CRT (intra-individualimprovement .25% in the Doppler-derived LV dP/dt). Among 40 patients, optimal cut-points predicting CRT responsewere 31% for LV apical rocking and 39% for AV-DYS. The presence of either apical rocking .31% or AV-DYS ≤39% had a sensitivity of 95%, specificity of 80%, positive predictive value of 83%, and a negativepredictive value of 94% for CRT response. Conclusion Afterpre-selection of candidates for CRT by QRS duration, application of a simple composite echocardiographic index mayexclude patients whowouldbe non-responders to CRT and thusimprove the global rate of therapy
% de temps en opposition Cutt of à 31% du RR %Avdys temps diastolique/RR *100
% Aprocking>31% % Av dys <36%