Download
1 / 134
1.38k likes | 1.63k Views
Pregnancy review. N. Petrenko, MD, PhD. Signs of pregnancy. Presumptive (generally subjective) Probable (objective) Positive (diagnostic). Presumptive symptoms of pregnancy ( felt by woman ):. Cessation of menses Nausea with or without vomiting “Morning sickness” Frequent urination

E N D
Pregnancyreview N. Petrenko, MD, PhD
Signs of pregnancy • Presumptive (generally subjective) • Probable (objective) • Positive (diagnostic)
Presumptive symptoms of pregnancy (felt by woman): • Cessation of menses • Nausea with or without vomiting • “Morning sickness” • Frequent urination • Fatigue • Breast tenderness, fullness, tingling • Maternal perception of fetal movement (“Quickening”) 18-20w, 16 w
Presumptive signs of pregnancy • Increased skin pigmentation – chloasma, linea nigra • Appearance of striae on abdomen and breasts
Probable signs of pregnancy (observedby examiner): • Changes in the size, shape, and consistency of the uterus (Hegar sign-softening of the cervix ) • Enlargement of the abdomen • Changes in the cervix (Goodell sign-softening of the cervix )
Probable signs of pregnancy (observedby examiner): • Bluish or purplish coloration of the vaginal mucosa and cervix (Chadwick’s sign-a dark blue to purplish-red congested appearance of the vaginal mucosa ) • Palpation of Braxton-Hicks contractions • Outlining the fetus manually • Endocrine tests of pregnancy
Positive signs of pregnancy(noted by examiner, confirm pregnancy) • Identification of the fetal heart beat separately and distinctly from that of the mother (10-12 w) • Perception of fetal movements by the examiner (18-20 w) • Visualization of pregnancy on ultrasound • Fetal recognition on X-ray
Gravida and Para • Gravida means a woman who has been, or currently is, pregnant • Para means a woman who has given birth • Nulligravida – never been pregnant • Primigravida – pregnant for the first time • Primipara – has delivered once • Multipara – has delivered more than once
G T P A L • G – GRAVIDA (how many pregnancies) • T – TERM (how many term deliveries) • P – PRETERM (how many preterm deliveries) • A – ABORTIONS (how many abortions, spontaneous or induced) • L – LIVING – how many children currently living
Term, Preterm, Abortion • TERM means delivery occurring in weeks 38-42 • PRETERM means delivery occurring in weeks 20-37 • ABORTION means delivery occurring before 20 weeks • POSTTERM means delivery occurring after week 42
Duration 280 days =40 weeks= 10 lunar months = 9 calendar month • 1st Trimester 1-13 weeks • Accepting reality of pregnancy • 2nd Trimester 14-26 weeks • Resolving feelings about her own mother; defining herself as a mother • 3rd Trimester 27-40 weeks • Active preparation for childbirth and baby
Assessment of Gestational Age • By LMP • By physical exam • By ultrasound
Nagele’s Rule • Subtract 3 months from that date then add 7 days • 1st day of LNMP (last normal menstrual period) Example: LNMP: September 10, 2006 Expected Due Date (EDD): June 17, 2007
Uterine Sizing • 6 weeks – globular with softening of the isthmus, size of a tangerine • 8 weeks – globular, size of a baseball • 10 weeks – globular with irregularity around one cornua (Piskacek’s sign), size of a softball • 12 weeks – globular, size of a grapefruit
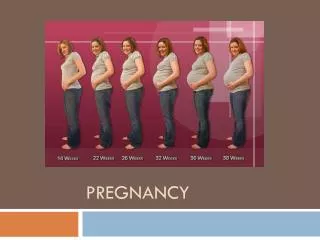
Uterine Sizing • Uterine enlargement • 12 weeks – At Symphysis • 16 weeks – Midway between symphysis and umbilicus • 20 weeks – At the umbilicus • 36 weeks - Near xyphoid process
Nausea with or without Vomiting • Starts at 4-6 weeks, peaks at 8-12 weeks, resolves by 14-16 weeks • Causes: unknown; may be rapidly increasing and high levels of estrogen, hCG, thyroxine; may have a psychological component • Rule out: hyperemesis gravidarum
Nausea and vomiting in early pregnancy • Most cases of nausea and vomiting in pregnancy will resolve spontaneously within 16 to 20 weeks of gestation. • Nausea and vomiting are not usually associated with a poor pregnancy outcome. A
Nausea and vomiting in early pregnancy • If a woman requests or would like to consider treatment, the following interventions appear to be effective in reducing symptoms: • non-pharmacological – ginger – P6 acupressure • pharmacological – antihistamines. A
Ptyalism • Excessive salivation accompanied by nausea and inability to swallow saliva • Cause: unknown; may be related to increased acidity in the mouth
Fatigue • Causes: unknown; may be related to gradual increase in BMR • Rule out: anemia, thyroid disease
Backache Women should be informed that exercising in water, massage therapy might help to ease backache during pregnancy. A
Upper Backache • Cause: increase in size and weight of the breasts • Relief: well-fitting, supportive bra
Low Backache • Cause: weight of the enlarging uterus causing exaggerated lumbar lordosis • Rule out: pyelonephritis (CVAT)
Leukorrhea • Definition: a profuse, thin or thick white vaginal discharge consisting of white blood cells, vaginal epithelial cells, and bacilli; acidic due to conversion of an increased amount of glycogen in vaginal epithelial cells into lactic acid by Doderlein’s bacilli • Rule out: vaginitis, STI, ruptured membranes
Urinary Frequency • 1st trimester: increased weight, softening of the isthmus, anteflexion of the uterus • 3rd trimester: pressure of the presenting part • Rule out: UTI
Heartburn • Relaxation of the cardiac sphincter due to progesterone • Decreased GI motility due to smooth muscle relaxation (progesterone) • Lack of functional room for the stomach because of its displacement and compression by the enlarging uterus • Rule out: GI disease
Heartburn • Women who present with symptoms of heartburn in pregnancy should be offered information regarding lifestyle and diet modification. • Antacids may be offered to women whose heartburn remains troublesome GPP A
Constipation • Decreased peristalsis due to relaxation of the smooth muscle of the large bowel under the influence of progesterone • Displacement of the bowel by the enlarging uterus • Administration of iron supplements
Constipation Women who present with constipation in pregnancy should be offered information regarding diet modification, such as bran or wheat fibre supplementation. A
Hemorrhoids • Relaxation of vein walls and smooth muscle of large bowel under influence of progesterone • Enlarging uterus causes increased pressure, impeding circulation and causing congestion in pelvic veins • Constipation
Hemorrhoids • Women should be offered information concerning diet modification. • If clinical symptoms remain troublesome, standard hemorrhoids creams should be considered. GPP
Leg Cramps • Cause: unknown. ? inadequate calcium, ? Imbalance in calcium-phosphorus ratio • Relief: straighten the leg and dorsiflex the foot:
Dependent Edema • Cause: impaired venous circulation and increased venous pressure in the lower extremities • Rule out: preeclampsia
Varicosities • Impaired venous circulation and increased venous pressure in lower extremities • Relaxation of vein walls and surrounding smooth muscle under the influence of progesterone • Increased blood volume • Familial predisposition
Varicose veins • Varicose veins are a common symptom of pregnancy that will not cause harm and • Compression stockings can improve the symptoms but will not prevent varicose veins from emerging. A
Insomnia • Discomfort of the enlarged uterus • Any of the common discomforts of pregnancy • Fetal activity • Psychological causes
Round Ligament Pain • Round ligaments attach on either side of the uterus just below and in front of insertion of fallopian tubes, cross the broad ligament in a fold of peritoneum, pass through the inguinal canal, insert in the anterior portion of the labia majora • When stretched, they hurt!
Screening for structural anomalies Pregnant women should be offered an ultrasound scan to screen for structural anomalies, ideally between 18 and 20 weeks’ gestation, by an appropriately trained sonographer and with equipment of an appropriate standard. A
Screening for Down’s syndrome Pregnant women should be offered screening for Down’s syndrome with a test which provides the current standard of a detection rate above 60% and a false-positive rate of less than 5%. B
The following tests meet this standard: • from 11 to 14 weeks – nuchal translucency (NT) – the combined test (NT, hCG and PAPP-A) • from 14 to 20 weeks – the triple test (hCG, AFP and uE3) – the quadruple test (hCG, AFP, uE3, inhibin A) B
Early pregnancy bleeding Spontaneous abortionIncompetent cervixEctopic pregnancyHydatiform mole
Abortion miscarriage • End of pregnancy before 20 weeks • Fetal weight less than 500 mg • Result of natural cause
miscarriage • 10-15% of recognize pregnancy end in miscarriage • Early (till 12 weeks) • before 8 weeks • 50% - result from chromosomal abnormalities • endocrine imbalance (luteal phase defects, insulin-dependent diabetes mellitus with high blood glucose levels in the first trimester), • immunologic factors (antiphospholipid antibodies), • Infections (bacteriuria and Chlamydia trachomatis), • Systemic disorders (lupus erythematosus), • genetic factors
miscarriage • Late 12 - 20 weeks • Result from maternal causes: • advancing maternal age and parity, • chronic infections, • premature dilation of the cervix and other anomalies of the reproductive tract, • chronic debilitating diseases, • nutrition, and recreational drug use
miscarriage • Little can be done to avoid genetically caused pregnancy loss, but correction of maternal disorders, immunization against infectious diseases, adequate early prenatal care, and treatment of pregnancy complications can do much to prevent miscarriage.