Download

1 / 39
390 likes | 553 Views
MUJER JOVEN CON CEFALEA Y DISMINUCIÓN DE LA AGUDEZA VISUAL. Vergara Díaz, MA; Gómez Rodríguez, P; Gómez Hernández, M; de la Rosa Morales, R; Espinosa Calleja, R; Blanco Torró, MD. Hospital San Juan de Dios del Aljarafe. Bormujos. Sevilla. ANTECEDENTES PERSONALES. No alergias medicamentosas.

E N D
MUJER JOVEN CON CEFALEA Y DISMINUCIÓN DE LA AGUDEZA VISUAL Vergara Díaz, MA; Gómez Rodríguez, P; Gómez Hernández, M; de la Rosa Morales, R; Espinosa Calleja, R; Blanco Torró, MD. Hospital San Juan de Dios del Aljarafe. Bormujos. Sevilla.
ANTECEDENTES PERSONALES • No alergias medicamentosas. • No hábitos tóxicos. • Síndrome Hipereosinofílico en la infancia. • Antecedentes familiares: - Madre: Esclerosis Múltiple - Padre: TBC pulmonar bacilífera (2009). • Estudio de convivientes PPD >20 mm → tratamiento con INH de forma irregular.
ENFERMEDAD ACTUAL CEFALEA FRONTAL + DISMINUCIÓN BRUSCA DE LA AGUDEZA VISUAL EN OJO IZQUIERDO 24 HORAS DE EVOLUCIÓN
EXPLORACIÓN FÍSICA • BEG, afebril, hemodinámicamente estable. • ACP: normal. Abdomen sin alteraciones. • MMII sin datos flogísticos ni lesiones cutáneas. • Exploración neurológica: sin alteraciones. • Campimetría de confrontación con déficit visual en OI.
PRUEBAS COMPLEMENTARIAS TAC CRANEAL (s/c) : • Asimetría entre lóbulos occipitales (posible origen connatal). No LOEs. • Calcificaciones distróficas en tienda del cerebelo derecha y de la hoz del cerebro. • Sinusitis etmoidal anterior bilateral y maxilar bilateral con nivel hidroaéreo.
ACTITUD INICIAL SERVICIO DE URGENCIAS CONSULTAS EXTERNAS OFTALMOLOGIA
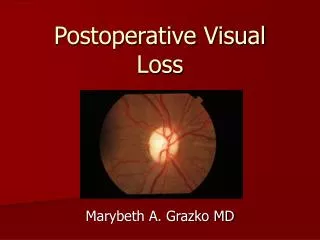
VALORACIÓN OFTALMOLOGICA (I) • AV: OI: Movimiento de manos. OD: 0.7. • FONDO DE OJO: • OI: Nódulos blanquecinos subretinianos (afectación macular). Neuritis prelaminar. • OD sin lesiones.
VALORACIÓN OFTALMOLOGICA (II) • Tomografía de Coherencia óptica (OCT): • OI: Lesiones hiperrefringentesintrarretinianas.
ACTITUD Hallazgos compatibles con CORIORRETINITIS MULTIFOCAL UNILATERAL Ingreso en MEDICINA INTERNApara estudio.
PRUEBAS COMPLEMENTARIAS (I) • Hemograma • Bioquímica (renal, hepático, cardíaco) • Sistemático de orina • Estudio de coagulación Leve eosinofília (500 cél/mm3) Resto normales/negativos
PRUEBAS COMPLEMENTARIAS (II) RX TÓRAX:
PRUEBAS COMPLEMENTARIAS (III) LCR : Acelular, sin consumo de glucosa, proteínas normales, ADA normal, citología y microbiología negativos.
EVOLUCIÓN • Revisión oftalmológica (a las 48 h del ingreso): - OD: Aparición de lesiones nodulares sin afectar mácula (AV: 0.6) - OI: Mismo aspecto clínico anterior (AV: 0.1).
EVOLUCIÓN • Revisión oftalmológica (a las 48 h del ingreso): ANGIOGRAFÍA: - OI: Lesiones parcheadas en polo posterior multifocales hiperfluorescentes. - OD: Lesiones hipoflurescentes en decusación vascular con una única lesión de centro hipercaptante.
JUICIO SINDRÓMICO Cuadro de CORIORRETINITIS AGUDA BILATERAL RÁPIDAMENTE PROGRESIVA
DIAGNÓSTICO DIFERENCIAL • Estudio de Humor vítreo. • Fondo de ojo/AFG: Coriorretinitis granulomatosa multifocal.
DIAGNÓSTICO DIFERENCIAL • Estudio de Humor vítreo. • Fondo de ojo/AFG: Coriorretinitis granulomatosa multifocal.
DIAGNÓSTICO DIFERENCIAL • No alteraciones articulares o dermatológicas. • FO: Neuritis prelaminar. • Rx tórax. • Punción lumbar. • ANA, ANCA, HLA B27, Anticoagulante lúpico. • Vit B12, VSG, FR. • NORMALES/ • NEGATIVOS
PRUEBAS COMPLEMENTARIAS RNM CRANEAL (c/ Gadolinio): • Lesiones de sustancia blanca supratentorial frontoparietal radiológicamente inespecífico.
PRUEBAS COMPLEMENTARIAS TAC tórax: • Discreta consolidación bronconeumónica en segmento apical (LSD), hasta región subpleural con alveolograma asociado y broncograma aéreo. • Patrón de perfusión en mosaico muy discreto con áreas de atrapamiento aéreo • (¿Enfermedad de la pequeña vía aérea?)
DIAGNÓSTICO DIFERENCIAL • Punción lumbar. • RNM craneal. • TAC craneal. • VSG, PCR, FR. • Proteinograma. • Marcadores tumorales. • NORMALES/ NEGATIVO
DIAGNÓSTICO DIFERENCIAL • Punción Lumbar • Rx y TAC tórax. • Serologías: Toxoplasma, CMV, VIH, LUES • Baciloscopia de esputo y orina • Cultivo de Lowestein • Fibrobroncoscopia, citología y aspirado. • PCR TBC, VHS y CMV en humor vítreo. • Serología IgG CMV +. • RESTO NORMALES/NEGATIVOS
DIAGNÓSTICO DIFERENCIAL • EPITELIOPATÍA PIGMENTARIA PLACOIDE AGUDA MULTIFOCAL • CORIORRETINITIS TUBERCULOSA PRIMARIA
PRUEBAS COMPLEMENTARIAS Mycobacterium tuberculosis Interferón-gamma (Quantiferón) en sangre total: POSITIVO
JUICIO CLÍNICO CORIORRETINITIS TUBERCULOSA PRIMARIA
TUBERCULOSIS PULMONAR EXTRAPULMONAR MILIAR • Ganglionar • Pleural • Genitourinaria • Osteoarticular • Meningitis • Digestiva • Pericarditis Primaria Postprimaria • Tubérculos coroideos • Neumonía con infiltrado microlobulillar • FOD • Hepatoesplenomegalia y linfadenopatías Otras formas extrapulmonares menos frecuentes: ORL, Ocular, Cutánea, Suprarrenaly Congénita
TBC OCULAR • Entidad poco frecuente. Incidencia: 1%. • Impacto no bien reconocido. • Puede comprometer cualquier componente del sistema visual. • La mayoría estos pacientes NO TIENEN HISTORIA de enfermedad pulmonar o sistémica • RX tórax normal (50% casos).
QUANTIFERÓN-TB • Ventajas: • S: 89.0% y E:98.1% • Detecta la infección tuberculosa latente. • Resultados disponibles <24 horas. • No sujeta a sesgos y errores de la colocación de TST y lectura. • No expone a las personas contra el antígeno. • No influenciado por vacunación BCG previa. • Inconvenientes: • Errores en la recogida o transporte de muestras de sangre e interpretación de la prueba puede disminuir precisión. • Puede ser positiva en TBC latente y en Enfermedad tuberculosa activa (interpretación en base a clínica).
TRATAMIENTO Durante el ingreso: • Isoniazida/Pirazinamida/Rifampicina 120/300/50 mg, 5 comp en ayunas cada 24 h. • Prednisona 50 mg cada 24 h. Al alta: • Retirada progresiva de tratamiento con Corticoides. • INH/Pirazinamida/Rifampicina 120/300/50 mg hasta próxima revisión.
EVOLUCIÓN • Revisión oftalmológica a 15 DÍAS del alta:Mejoría de la agudeza visual (OI: 0.3, OD: 0.5). Ausencia de signos inflamatorios. FO con signos de dispersión pigmentaria tipo cicatriz. • Revisión 1er MES del alta:Evolución favorable. No efectos tóxicos de la medicación.
EVOLUCIÓN • Revisión a los 3 MESES del alta: • Áreas de atrofia y dispersión de epitelio pigmentario. • OI: afectación fóvea. AV: 0.5 • OD: afectación extrafoveal. AV: 0.6. • Tto: Rifampizina 300 + Isoniazida 150 mg (2 comp/d )
JUICIO CLÍNICO CORIORRETINITIS TUBERCULOSA PRIMARIA
BlBLIOGRAFÍA • Arias Guillén A. Avances en el diagnóstico de la infección tuberculosa. Arch. Bronconeumol. 2011;47 (10): 521-530. • Hang NTL, Lien LT, Kobayashi N, Shimbo T, Sakurada S, et al. (2011) Analysis of FactorsLoweringSensitivity of interferon-y ReleaseAssayfor Tuberculosis. PLoS ONE 6 (8): e23806. doi:10.1371/journal.pone.0023806. • Nienhaus et al.: Systematicreview of cost and cost-effectiveness of different TB-screeningstrategies. BMC HealthServicesResearch 2011 11:247. • Lu C, Wu J, Wang H, Wang S, Diao N, et al. (2011) Novel BiomarkersDistinguishing Active Tuberculosis fromLatentInfectionIdentifiedby Gene. Expression Profile of Peripheral Blood Mononuclear Cells. PLoS ONE 6(8): e24290. doi:10.1371/journal.pone.0024290. • Samimi S. , Renaud-Rougier MB, Delyfer MN, Korobelnik JF. Dosage plasmatique de l’interféron gamma comme moyen diagnostique en cas de tuberculose oculaire isolée. Journal français d’ophtalmologie (2009) 32, 411—414. • De Benedetti ME, Carranza B, Gotuzzo E, Rolando I. Tuberculosisocular. Rev. Chil Infect 2007; 24 (4): 284-295. • Hougardy J-M, Schepers K, Place S, Drowart A, Lechevin V, et al (2007) Heparin-Binding-Hemagglutinin-Induced IFN-c Release as a Diagnostic. Tool for Latent Tuberculosis. PLoS ONE 2(10): e926. doi:10.1371/journal.pone.0000926. • Thompson MJ, Albert DM. Ocular Tuberculosis. Arch Ophthalmol. 2005;123:844-9. • Ortega G, Bobadilla del Valle M, Ponce de León A, Sifuentes J. NestedpolymerasechainreactionforMycobacterium tuberculosis DNA detection in aqueous and Vitreous of patientswithuveitis. Archives of MedicalResearch; 2003;34;116-119.