Download
1 / 44
490 likes | 616 Views
Dive into the complex cellular events of leukocyte recruitment and activation in inflammation. Learn about the steps involved, from margination and rolling along vessels to emigration, chemotaxis, and phagocytosis. Explore the molecules, adhesion, and chemotactic agents crucial in this inflammatory response.

E N D
Inflammation Dr. Ahmad Hameed MBBS,DCP, M.Phil
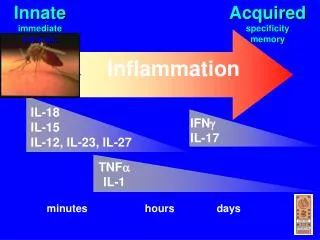
Cellular Events: Leukocyte Recruitment and activation Leukocyte recruitment • Margi nation and rolling along the vessel • Firm adhesion to the endothelium • Transmigration between endothelial cells • Migration in interstitial tissues toward a chemo tactic stimulus
Margination and Rolling • With increased vascular permeability, fluid leaves the vessel causing leukocytes to settle-out of the central flow column and “marginate” along the endothelial surface • Endothelial cells and leukocytes have complementary surface adhesion molecules which briefly stick and release causing the leukocyte to roll along the endothelium like a tumbleweed until it eventually comes to a stop as mutual adhesion reaches a peak
Margination and Rolling • Early rolling adhesion mediated by selectin family: • E-selectin (endothelium) • P-selectin (platelets, endothelium) • L-selectin (leukocytes) • Bind surface molecules (i.e.,CD34, Sialyl-Lewis X-modified GP) that are up regulated on endothelium by cytokines (TNF, IL-1) at injury sites
Emigration of leukocytes: margination, rolling, adhesion, diapedesis, migrationNeutrophils predominate (6-24 hours) and replaced by Monocytes (24-48 hours)Upregulation of molecules • E-selectin (endothelium) - rolling, adhesion [induced by IL-1 and TNF]P-selectin (endothelium, platelets) - rolling [present in Weibel-Palade bodies]L-selectin (leukocytes) - homing
Adhesion • Rolling comes to a stop and adhesion results • Other sets of adhesion molecules participate: • Endothelial: ICAM-1, VCAM-1 • Leukocyte: LFA-1, Mac-1, VLA-4 (ICAM-1 binds LFA-1/Mac-1, VCAM-1 binds VLA-4) • Ordinarily down-regulated or in an inactive conformation, but inflammation alters this by chemokines along with cytokines e.g. IL-1, TNF
ICAM (interacts with integrins LFA-1 on leukocytes) adhesion, arrest, transmigration • VCAM (interacts with integrins on eos, monos, lymphs) adhesion • PECAM-1 (CD31) platelet-endothelial cell adhesion molecule • Upon stimulation by chemokinesintegrins undergo conformational changes and cluster together with high affinity
Emigration and chemotaxis • Emigrationis a mechanism by which the leukocytes extend pseudopodia, pass through the capillary walls by ameboid movement, and migrate into the tissue spaces. • The emigration of leukocytes also may be accompanied by an escape of red blood cells. • Once they have exited the capillary, the leukocytes move through the tissue guided by secreted cytokines, bacterial and cellular debris, and complement fragments (C3a, C5a). • The process by which leukocytes migrate in response to a chemical signal is called chemotaxis.
Transmigration • Leukocytes migrate through vessel wall by squeezing between cells at intercellular junctions (diapedesis) • Occurs mainly within the systemic venules and pulmonary capillaries via PECAM –1 (platelet endothelial adhesion molecule 1) (CD31). It is expressed on both leukocytes and endothelial cells. • Must then cross basement membrane by collagenases • Early in inflammatory response mostly PMNs, but as cytokine and chemotactic signals change with progression of inflammatory response, alteration of endothelial cell adhesion molecule expression activates other populations of leukocytes to adhere (monocytes, lymphocytes, etc)
Chemotaxis • Leukocytes follow chemical gradient to site of injury (chemotaxis) • Soluble bacterial products (N-formylmethionine peptides) • Complement components (C5a) • Cytokines (chemokine family e.g., IL-8) • LTB4 (AA metabolite) • Chemotactic agents bind surface receptors (G protein-coupled receptors) signal transduction influx of calcium assembly of cytoskeletal contractile elements. • Leukocytes extend pseudopods with overlying surface adhesion molecules (integrins) that bind ECM during chemotaxis which pulls the leukocyte in direction of attachment
Chemotaxis • In acute inflammation neutrophils predominate in the inflammatory infiltrate during the first 6 to 24 hours and are replaced by monocytes in 24 to 48 hours. • Most numerous leukocytes • Attach more firmly to the adhesion molecules • Neutrophils are short live-they die by apotosis and disappear within 24 to 48 hours. • Monocytes survive longer
Leukocyte Activation • Leukocyte activation results in the enhancement • Phagocytosis of particles • Intracellular destruction of phagocytosed microbes and dead issues • Liberation of substances that destroy extracellular microbes and dead tissues • Production of mediators
Phagocytosis • During the next and final stage of the cellular response, the neutrophils and macrophages engulf and degrade the bacteria and cellular debris in a process called phagocytosis. • Phagocytosis involves three distinct steps: • Recognition and attachment of the particle to the ingesting leukocyte • Engulfment, with subsequent formation of a phagocytic vacuole • Killing and degradation of the ingested material • If the antigen is coated with antibody or complement, its adherence is increased because of binding to complement. This process of enhanced binding of an antigen caused by antibody or complement is called opsonization.
Phagocytosis • Recognition and attachment via opsonization (Fc fragment of IgG, C3b, collectins)· • Engulfment via binding of the opsonized particle to the FcγR • Corresponding receptors on leukocytes (FcR, CR1, 2, C1q) leads to binding
Killing and Degradation of Phagocytosed Microbes • Triggers an oxidative burst ,engulfment and formation of vacuole which fuses with lysosomal granule membrane (phagolysosome) • Granules discharge within phagolysosome and extracellularly (degranulation) • The most imp. Microbicidal substances are ROS and lysosomal enzymes.
Oxidative burst • Phagocytosis stimulates an Oxidative burst charecterized by • Increase in oxygen consumption • Glycogenolysis • Increase glucose oxidation • Production of ROS • Formation of superoxide ion • 2O2 + NADPH 2O2-rad + NADP+ + H+ (NADPH oxidase) • O2 + 2H+ H2O2(dismutase)
Reactive oxygen species • Hydrogen peroxide alone insufficient • MPO (azurophilic granules) converts hydrogen peroxide to HOCl- (in presence of Cl- ), an oxidant/antimicrobial agent • Therefore, PMNs can kill by halogenation, or lipid/protein peroxidation
Degradation and Clean-up • Reactive end-products only active within phagolysosome • Hydrogen peroxide broken down to water and oxygen by catalase • Dead microorganisms degraded by lysosomal acid hydrolases
Leukocyte granules • Other antimicrobials in leukocyte granules: • Bactericidal permeability increasing protein (BPI) • Lysozyme • Lactoferrin • Defensins (punch holes in membranes)
Secretion of Microbicidal Substances • Leukocytes also secrete elastase which destroy and digest extracellular microbes and dead tissues, as well as antimicrobial peptides. • Phagocytic vacuole may remain transiently open to the outside before complete closure of the phagolysosome (regurgitation during feeding). • If cells encounter materials that cannot be easily ingested, such as immune complexes deposited on immovable surfaces (e.g. glomerular basement membrance). Attempt to phagocytose these substances (frustrated phagocytosis) triggers strong leukocyte activation • The membrance of the phagolysosome may be damaged if potentially injurious substances.
Neutrophil Extracellular Trapes (NETs) • Neutrophils These traps are extracellular fibrillar networks that are produced by neutrophils in response to infectious pathogens, inflammatory mediators • Contain a framework of nuclear chormatin with embedded granule proteins, such as antimicrobial peptides and enzymes • The traps provide a high concentration of the antimicrobial substances at sites of infection, and prevent the spread of the microbes by trapping them in the fibrills. In the process, the nuclei of the neutrophils are lost, leading to death of the cells. NETs also have been detected in blood neutrophils during sepsis.
Leukocyte-Induced Tissue Injury • Because leukocytes secrete harmful substances e.g. enzymes , ROS, they are important cause of injury to normal cells and tissues under several circumstances • “Bystander tissues” are injured. • In tuberculosis and some viral diseases , contributes more to the pathologic process than does the microbe itself • As a normal attempt to clear damaged and dead tissues (e.g. myocardial infarction). In an infarct, inflammation may prolong and exacerbate the injurious consequences of the ischemia • When the inflammatory response is inappropriately directed against host tissues, as in certain autoimmune diseases, or when the host reacts excessively against nontoxic environmental substances, such as asthma • Activated leukocytes, especially macrophages, also secrete may cytokines, which stimulate further inflammation and have important systemic effects
Defects in leukocyte function • Defects of adhesion: • In LAD-1: LFA-1 and Mac-1 subunit defects lead to impaired adhesion • In LAD-2: Absence of sialyl-Lewis X, and defect in E- and P-selectin sugar epitopes • Defects in phagolysosome formation • Microtubule assembly defect leads to impaired locomotion and lysosomaldegranulation (Chediak-Higashi Syndrome) • Defects of microbicidal activity: • Deficiency of phagocyte oxidase that generates ROS, therefore no oxygen-dependent killing mechanism (chronic granulomatous disease)
OUTCOMES OF ACUTE INFLAMMATION • 1) RESOLUTION • 2) SCARRING • 3)CHRONIC inflammation
Resolution • The complete restoration of the inflamed tissue back to A normal status. Inflammatory measures such as vasodilation, chemical production, and leukocyte infiltration cease, and damaged parenchymal cells regenerate. In situations where limited or short lived inflammation has occurred this is usually the outcome.
Fibrosis • Large amounts of tissue destruction, or damage in tissues unable to regenerate, can not be regenerated completely by the body. Fibrous scarring occurs in these areas of damage, forming a scar composed primarily of collagen. The scar will not contain any specialized structures, such as parenchymal cells, hence functional impairment may occur.
Chronic inflammation • In acute inflammation, if the injurious agent persists then chronic inflammation will ensue. This process, marked by inflammation lasting many days, months or even years, may lead to the formation of a chronic wound. Chronic inflammation is characterised by the dominating presence ofmacrophages in the injured tissue. These cells are powerful defensive agents but the toxins they release are injurious to the organism's own tissues Consequently, chronic inflammation is almost always accompanied by tissue destruction.
Outcomes of acute inflammation: resolution, healing by scarring (fibrosis), or chronic inflammation.
Morphologic Patterns of Acute Inflammation • Serous inflammation • Charterised by Watery relatively protein-poor fluid • Derived from the plasma or secretions of mesothelial cells lining the peritoneal, pleural, and pericardial cavities. • Skin blister • Fluid in a serous cavity is called an effusion
Serous inflammation. Low-power view of a cross-section of a skin blister showing the epidermis separated from the dermis by a focal collection of serous effusion.
Morphologic Patterns of Acute Inflammation • Fibrinous inflammation • Occurs as a consequence of severe injuries, resulting in greater vascular permeability that allows large molecules such as fibriongen to pass the endothelial barrier • A fibrinousexudate is charcteristic of inflammation in the lining of body cavities, such as the meninges pericardium, and pleura • Such exudate is degraded by fibrinolysis, and the accumulated debris may be removed by macrophages resulting in restoration of the normal tissue structure (restoration) • Organization
Fibrinous pericarditis. A, Deposits of fibrin on the pericardium. B, A pink meshwork of fibrin exudate (F) overlies the pericardial surface (P).
Morphologic Patterns of Acute Inflammation • Suppurative (purulent) inflammation and abscess formation • Collection of purulent exudate (pus) consisting of neutrophils, necrotic cells, and edermafludi. Certain organisms e.g. staphylococci are more likely to induce such localized suppuration and are therefore pyogenic pus forming • Abscesses: Focal collection of pus caused by pyogenic organisms into a tissue or by secondary infections of necrotic foci. • Abscesses typically have a central, largely necrotic region rimmed by a layer rimmed by a layer of neutrophils, dialatedvesseles and fibrobalstprolification • As time passes, the absess may become completely walled off and eventually be replaced by connective tissue. • Because of the underlying tissue destruction, the usual outcome with abscess formation is scarring
Purulent - Inflammation - PUS • Purulent inflammation with abscess formation. A, Multiple bacterial abscesses in the lung (arrows) in a case of bronchopneumonia. • B, The abscess contains neutrophils and cellular debris and is surrounded by congested blood vessels.
PUS = PURULENT ABSCESS = POCKET OF PUS = NEUTROPHILS
Morphologic Patterns of Acute Inflammation • Ulcer is a local defect, or excavation, of the surface of an organ or tissue that is produced by necrosis of cells and sloughing (shedding) of necrotic and inflammatory tissue. • Inflammation exist on or near a surface. Ulcer are most commonly encountered in the mucosa of a mouth, stomach, intestines, or genitourinay tract and (2) in the subcutaneous tissues of lower extremities in older persons who have circulation disturbances predisposing affected tissue to extensive necrosis. Ulcerations are best exemplified by peptic ulcer of the stomach or duodenum, in which acute and chronic inflammation coexist.
Ulcer. A, A chronic duodenal ulcer. B, Low-power crosssection of a duodenal ulcer crater with an acute inflammatory exudate in the base.