Download
1 / 39
390 likes | 686 Views
Prof. Pavlyshyn H.A. ACUTE RHEUMATIC FEVER. DEFINITION. Rheumatic fever is an inflammatory process which can involve the joints, heart, skin and brain It is caused by antibody cross reactivity and occurs 2-3 weeks after a Group A Streptococcal infection. EPIDEMIOLOGY.

E N D
Prof. Pavlyshyn H.A. ACUTE RHEUMATIC FEVER
DEFINITION Rheumatic fever is an inflammatory process which can involve the joints, heart, skin and brain It is caused by antibody cross reactivity and occurs 2-3 weeks after a Group A Streptococcal infection.
EPIDEMIOLOGY • 470,000 new cases of Acute Rheumatic Fever/year • 233,000 deaths due to Rheumatic Fever/year • Majority of deaths occur in developing countries • Incidence in the US: 2-14 cases/100,000 • Historically, there is a temporal relationship between epidemics of streptococcal pharyngitis and scarlet fever with the epidemics of acute rheumatic fever • No clear gender predilection overall, but mitral stenosis and syndenham’s chorea occur more in females than males.
BACKGROUND Primarily affects children between ages 5-12 Generally occurs 2-3 weeks after Group A Streptococcal infection (strep throat or scarlet fever) In the US, Rheumatic fever has become fairly rare due to use of antibiotics to treat streptococcal infections Globally, 3% of those with an untreated streptococcal infection develop rheumatic fever 40% of those with Acute Rheumatic Fever develop mitral stenosis as adults
BACKGROUND Cutaneous streptococcal infections have not been shown to initiate Acute Rheumatic Fever. Strains of certain M serotypes/genotypes of streptococci have higher associations than other genotypes Epidemics of Acute Rheumatic Fever in Trinidad and Chile showed that streptococci causing Acute Rheumatic Fever belonged to different serotypes than those that cause Acute Glomerulonephritis.
PATHOPHYSIOLOGY • Exact mechanism of how Group A streptococcal infection causes Acute Rheumatic Fever is unknown however it is believed to be caused by a cross reactivity of antibodies • Suggested Theories • Toxic effects of streptococcal products (streptolysin S or O) which then cause direct tissue injury • Serum Sickness-like reaction mediated by antigen-antibody complexes • Autoimmune phenomenon
PATHOPHYSIOLOGY More support for an autoimmune phenomenon (Type II hypersensitivity reaction) During strep infection, antigen presenting cells present bacterial antigen to helper T cells. These helper T cells then activate B cells to induce production of antibodies against the Streptococcal cell wall. These antibodies can also interact with other cells in the body (for example, myocardium or joints, etc) producing the symptoms responsible with acute rheumatic fever
PATHOGENESIS • Most patient have elevated antibody titers to at least one streptococcal antibody • Streptolysin O • Hyaluronidase • Streptokinase
PATHOPHYSIOLOGY (CARDIAC) Aschoff nodule with owl-eyed shape in the cross section and catapillar-shaped in the longitudinal section
PATHOPHYSIOLOGY (CARDIAC) Thickened fused chordae of the mitral valve
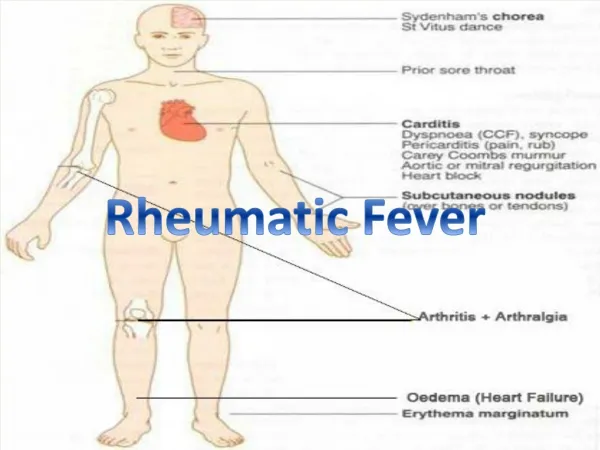
CLINICAL MANIFESTATIONS Latent period: time between preceding streptococcal pharyngitis and Acute Rheumatic fever is about 19 days (range 1-5 weeks) If initial complaint is polyarthritis, disease generally has more abrupt onset compared to if initial presentation is with myocarditis. Arthritis occurs in 75% of initial attacks, carditis in 40-50% and chorea in 15% with subcutaneous nodules and erythema marginatum in <10%
CLINICAL MANIFESTATIONS (CARDITIS) • Usually manifests within the first 3 weeks of Acute Rheumatic Fever • Signs: new heart murmur, cardiomegaly, CHF, perciardial friction rub, effusions • Chronic inflammatory changes may lead to development of rheumatic heart disease. • Characteristic murmur or Rheumatic heart disease: • mitral regurgitation • Low-pitched mid diastolic flow murmur at the apex (Carey Coombs murmur • Aortic regurgitation • Can also get AV conduction delays
CLINICAL MANIFESTATIONS (JOINTS) Arthralgias and arthritis (may be migratory) Warm, swollen, tender joints Usually involves the knees, ankles, elbows and wrists Lasts 2-3 weeks
CLINICAL MANIFESTATIONS • Subcutaneous Nodules: usually associated with severe carditis and occur several weeks after onset. • Firm, painless nodules (up to 2cm) found over bony surfaces and tendons • Occur near elbows, knees, wrists, achilles tendon, vertebral joints • Usually persist for 1-2 weeks
CLINICAL MANIFESTATIONS • Erythema Marginatum: nonpruritic, painless erythematous rash on trunk and/or proximal extremities • Macular lesions with raised margins and central clearing • May last from weeks to months
CLINICAL MANIFESTATIONS • Sydenham’s Chorea: neurologic disorder with muscular weakness, emotional lability and involuntary, uncoordinated, purposeless movements • Disappear during sleep • Mainly occur in hands, feet and face • Sensation intact • Lasts 2-4 months
DIFFERENTIAL DIAGNOSIS Poststreptococcal reactive arthritis: is non-migratory Rheumatoid Arthritis SLE Infective endocarditis Sickle Cell disease Drug reactions TB Lyme Disease Serum Sickness
DIAGNOSIS • JONES CRITERIA • Developed by Dr. T Duckett Jones in 1944 • Need 2 major criteria or 1 major and 2 minor criteria in the presence of a prior strep infection to make the diagnosis • Evidence of prior strep infection with positive throat culture or antigen test, elevated streptococcal antibody titer, or history of rheumatic fever/heart disease
MAJOR CRITERIA • Migratory Polyarthritis: migrating arthritis with inflammation involving the large joints (knees, ankles, elbows, wrists) and typically affects the leg joints first • Carditis: can manifest with new murmur, pericarditis, congestive heart failure • Subcutaneous Nodules: a form of aschoff bodies. Are painless nodules on the back of the wrists, elbows, knees • ErythemaMarginatum: rash beginning on the arms or trunk and spreads outward. Lesion with ring with central clearing. Worsens with heat. Does not involve the face • Sydenham’s Chorea (St. Vitus’ Dance): purposeless movements of the face and arms. Late finding
MINOR CRITERIA Fever Arthralgia: joint pain without inflammation Elevated CRP, ESR or leukocytosis EKG changes: primarily prolonged PR interval Evidence of Group A Streptococcal infection via elevated antistreptolysin O titer or DNAase Prior history of rheumatic fever or heart disease
TREATMENT Anti-inflammatory Agents Antibiotics Prophylaxis
ANTI-INFLAMMATORY AGENTS Aspirin 4-8grams/day for adults Continue anti-inflammatory therapy until ESR or CRP are normal May need steroids if there is cardiac involvement to help prevent sequelae such as mitral stenosis Corticosteroids, if indicated, are given at prednisone 2mg/kg/day for 2 weeks and then tapered
ANTIBIOTICS Penicillin for at least 10 days Penicillin 500mg BID-TID Can use erythromycin for PCN allergic patients (given at 40mg/kg/day given in 2-4 doses/day)
PROPHYLAXIS • Prophylaxis needed to prevent recurrence of Acute Rheumatic Fever • Start prophylaxis after acute episode resolves • Can use: • Penicillin V 250mg BID or, • Sulfadiazine 1000mg daily, or • Penicillin G 1.2 million units IM q4weeks • For PCN allergic patients: erythromycin 250mg PO BID • Recurrence of disease generally occurs in the first couple years
PROPHYLAXIS • WHO GUIDELINES • At least 5 years of prophylaxis or if child until age 18 if not cardiac involvement • 10 years prophylaxis or if child until age 25 if has mild mitral regurgitation • Lifelong prophylaxis if has severe valve disease