Rheumatic Fever
270 likes | 343 Views
Rheumatic Fever. Prof SC Brown M.MeD FCP (paed, cardio) DCH. How common is RHD?. 2 -3 % of infected GABHS RF WHO 15.6 mill RHD 300 000 of 0.5mill ARF > RHD p.a. 233 000 deaths p.a. Prevalence Sub Saharan Africa 5.7/1000 in children 5 – 14y Asia 2 – 3.5/100 Developed countries

Rheumatic Fever
E N D
Presentation Transcript
Rheumatic Fever Prof SC Brown M.MeD FCP (paed, cardio) DCH
How common is RHD? • 2 -3 % of infected GABHS RF • WHO • 15.6 mill RHD • 300 000 of 0.5mill ARF > RHD p.a. • 233 000 deaths p.a. • Prevalence • Sub Saharan Africa • 5.7/1000 in children 5 – 14y • Asia • 2 – 3.5/100 • Developed countries • 0.5/1000 • Characteristics • Rare at young age (< 5% younger 5y) • F > m
Incidence ARF & RHD in Aboriginal Australians – Dpt of Health and community services, Northern Australia 400 35 RHD 2003 Incidence of ARF per 1000 200 Prevalence RHD per 1000 15 ARF 2002 < 5 5-14 15-24 25-34 > 34
Natural progression of rheumatic fever Rx First contact with Streptococcus 5 – 15 yr Acute RF arthritis fever carditis skin I/T 2 – 3 w pharyngitis Prophylaxis! Jones criteria Jones criteria Relapse / acute on chronic Chronic RF MR, AR years MS, AS
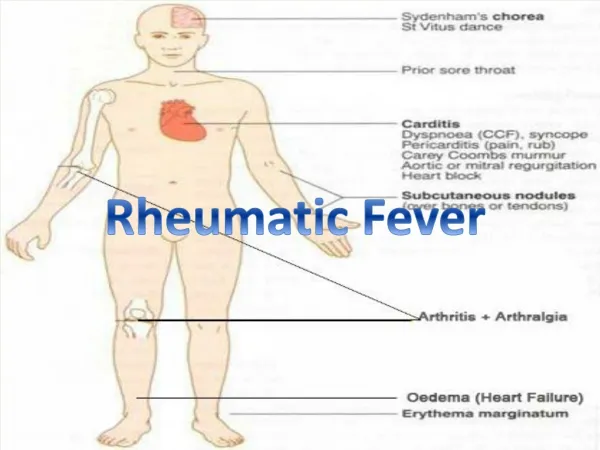
MAJOR fleeting poliarhtritis carditis erythema marginatum subcut nodules Sydenhams chorea MINOR history of previous RF arthralgia fever PR prolongation - ECG LAB WCC, ESR, CRP JONES CRITERIA: PLUS • EVIDENCE OF RECENT STREPTOCOCCAL INFECTION e.g. ASOT
Drug Therapy anti-inflammatory antibiotics prevention
Treatment • not all tested in controlled trials • e.g. longterm bedrest for carditis • e.g. Pen for URTI • Not affect cardiac outcome after 1 y • anti-inflammatory • antibiotics
Anti-inflammatory • Salicylates • rapid resolution fever, arthritis, arhtralgia • evidence: • NOT be used carditis • do not decrease incidence of residual RHD • Dorfman (Pediatrics 1961): 12 week aspirin similar incidence of murmurs as controls > 1yr • meta analysis Cochrane 2003,CD003176) • No benefit over steroid or vice versa • indication • symptomatic Rx of fever, arthritis, arthralgia
Anti-inflammatory • steroids • reduce inflammatory response of ARF • esp. fever & acute phase reagents • little objective evidence • studies done before ECHO • meta-analyses no benefit over salisylates or placebo of RHD after 1 –10 y • most > 40y ago • not test newer corticosteroids
Anti-inflammatory: other • NSAIDS • Naproxen in 1 small trial • Immunoglobulins • IVIG in ARF – no diff > 1y • Chorea • Rx reserved moderate-severe symptoms • Valproic acid > carbamazepine or haloperidol • PROBLEM • need studies • natural progression of RHD • 60% regress after 10y
Prevention • oral • once daily amoxycillin • high dose amoxycillin • azithromycin • not recommended by US • intravenous • 3 - 4weekly • practical aspects • small gauge needles • 1% lignocaine or procaine penicillin • slow injection(3min) • direct pressure and warming of medication (room temp)
prevention • treat carriers & children with sore throat • 1965 • possible reduction ARF 21% • cost US $12 pa per child or $65 000 per ARF prevented • New Zealand • school based sore throat diagnosis & treatment • no reduction in ARF incidence • programmes not practical or affordable • vaccine • multivalent vs M-serotype • unlikely < 2015
Subclinical Rheumatic carditis • “silent” mitral regurgutation ECHO • MR jet > 1 • MR in 2 planes • velocity > 2,5m/s • chorea & arthritis: silent MR • abn valve – murmur 2w or 18mo -5y or MS • studies • trivial MR 45% normal children • ? higher in febrile patients • New Zealand study • Affect diagnosis of ARF in 10% of cases • summarise • controversial • problems with Echocardiography • WHO addition to Jones criteria justified
role of ECHO • normal population • MR : 2,4 – 50% • AR : 0 – 33% • TR : 6,3 – 95% • PR : 21.9 – 92% • rheumatic fever • excludes nonrheumatic causes • e.g. prolapse, bicuspid aov • acute carditis • 25% nodules tip leaflets, disappear follow-up • classification of severity • 1+ to 4+ • no murmur • later develop RHD
Indications for referral to surgical centre (WHO) • symptoms have progressed beyond New York Heart Association(NYHA) Class II. Note: with aortic stenosis (AS), all symptomatic patients should be referred. • patients who are asymptomatic, or mildly symptomatic, with progressive left ventricular enlargement on clinical or radiological examination (>0.5 cm/year). • cardiac failure due to the valve lesion itself, rather than to an episode of rheumatic carditis. • Pulmonary hypertension, with physical signs and ECG evidence of changes in right ventricular hypertrophy, and chest X-ray evidence of pulmonary artery dilatation. • tricuspid regurgitation that complicates mitral valve disease. • development of atrial fibrillation. • thromboembolism. • endocarditis is suspected to contribute to cardiac decompensation.
surgery during acute phase n = 254 MR + HF age: 6 – 52y rheumatic activity : n = 76 higher incidence of early cx 5 ± 3y 47% acute mortality: 2.6% 5y mortality: 15% re-operation 27% conclusion “surgical valve repair during active carditis was associated with an acceptable survival rate, but reoperations were frequent” Circulation, 1994,90(5 Pt 2):II 167–174.
surgery during acute phase: conclusions • surgery can be safely performed during active carditis and, in of active carditis, may be preferable to the long-term use of corticosteroids. • myocardial inflammation plays no significant role in the clinical pathology of active carditis. • valve repair during active carditis may not constitute the best surgical option if there is macroscopic evidence of valvular inflammation, because valve repair is associated with significant reoperation rates.
conclusion • ? are we missing ARF • pathogenesis – answers • Jones criteria • challenge old ideas WHO Expert Consultation on Rheumatic Fever and Rheumatic Heart Disease (2001 : Geneva, Switzerland) Rheumatic fever and rheumatic heart disease