Download
1 / 25
250 likes | 400 Views
ASCO 07, June 3rd. ADVANCED PANCREATIC CANCER TREATMENT : NOTHING NEW ??. Christophe Louvet Hôpital St-Antoine Paris, France. The Burris Study. Gemcitabine. 5-Fluorouracil. n=63. n=63. 23.8% *. 4.8%. Clinical Benefit. Median Survival. 5.65 months **. 4.41 months. * p = 0.0022.

E N D
ASCO 07, June 3rd. ADVANCED PANCREATIC CANCER TREATMENT : NOTHING NEW ?? Christophe Louvet Hôpital St-Antoine Paris, France
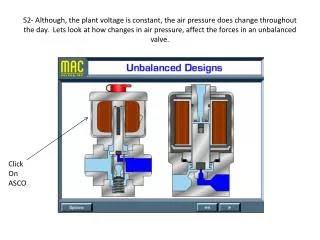
The Burris Study Gemcitabine 5-Fluorouracil n=63 n=63 23.8% * 4.8% Clinical Benefit Median Survival 5.65 months ** 4.41 months * p = 0.0022 ** p = 0.0025 Burris H A, et al.: JCO 15: 2403, 1997
Gem ± 5FU bolus (Berlin, 2002) 3.4 6.7 Gem ± Capecitabine (Herrmann, 2005) 4.8 8.4 Gem ± 5FU/LV (Riess, 2005) 4.9 5.9 Gem ± Capecitabine (Cunningham, 2005)-7.4 Gem ± Marimasmat (Bramhall, 2002) NA 5.5 Gem ± Tifarbinib (Van Cutsem, 2004) 3.7 6.4 Gem ± Exatecan (O’Reilly, 2004) 3.7 6.7 Gem ± CPT-11 (Rocha-Lima, 2004) 3.4 6.3 Gem ± Pemetrexed (Richards, 2004) 3.3 6.2 Randomized phases III in Pancreatic Cancer Study PFS/TTP(m) OS (m) Study PFS/TTP(m) OS (m)
Median survival 12-month (months, 95%CI) survival GEM 6.0 (5.4, 7.1) 19% GEM-CAP 7.4 (6.5, 8.5) 26% Hazard Ratio: 0.80 (95% CI: 0.65, 0.98) Log rank p=0.026; χ2LR=4.93 Gem ± Capecitabine
Gem ± 5FU bolus (Berlin, 2002) 3.4 6.7 Gem ± Capecitabine (Herrmann, 2005) 4.8 8.4 Gem ± 5FU/LV (Riess, 2005) 4.9 5.9 Gem ± Capecitabine (Cunningham, 2005)-7.4 Gem ± Cisplatin (Heinemann, 2003) 5.3 7.5 Gem ± Oxaliplatin (Louvet, 2004) 5.89.0 Gem ± Oxaliplatin (Poplin, 2006) - 5.9 Gem ± Marimasmat (Bramhall, 2002) NA 5.5 Gem ± Tifarbinib (Van Cutsem, 2004) 3.7 6.4 Gem ± Exatecan (O’Reilly, 2004) 3.7 6.7 Gem ± CPT-11 (Rocha-Lima, 2004) 3.4 6.3 Gem ± Pemetrexed (Richards, 2004) 3.3 6.2 Randomized phases III in Pancreatic Cancer Study PFS/TTP(m) OS (m) Study PFS/TTP(m) OS (m)
p Gem Gemox median 7.1 m 9.0 m 6-mth 60.4% 68.0% 8-mth45.3% 56.5% 9-mth 40.0% 48.1% 1-yr 27.8% 34.7% 0.13 GEM-GEMOX Study : Overall survival Overall Survival 1.0 Gem 0.9 Gemox 0.8 0.7 0.6 % survival 0.5 0.4 0.3 0.2 0.1 0.0 0 26 52 78 104 130 156 weeks Louvet C, et al. J Clin Oncol, 2005
ECOG Study (2006) Gem : median = 4.9 months Gemox : median = 5.9 months Gem FDR : median = 6.0 months Gem vs Gemox : NS Gem vs Gem FDR : NS GEM FDR GEMOX
Gem ± 5FU bolus (Berlin, 2002) 3.4 6.7 Gem ± Capecitabine (Herrmann, 2005) 4.8 8.4 Gem ± 5FU/LV (Riess, 2005) 4.9 5.9 Gem ± Capecitabine (Cunningham, 2005)-7.4 Gem ± Cisplatin (Heinemann, 2003) 5.3 7.5 Gem ± Oxaliplatin (Louvet, 2004) 5.89.0 Gem ± Oxaliplatin (Poplin, 2006) - 5.9 Gem ± Marimasmat (Bramhall, 2002) NA 5.5 Gem ± Tifarbinib (Van Cutsem, 2004) 3.7 6.4 Gem ± Exatecan (O’Reilly, 2004) 3.7 6.7 Gem ± CPT-11 (Rocha-Lima, 2004) 3.4 6.3 Gem ± Pemetrexed (Richards, 2004) 3.3 6.2 Randomized phases III in Pancreatic Cancer Study PFS/TTP(m) OS (m) Study PFS/TTP(m) OS (m) Gem ± Erlotinib (Moore, 2005) 3.7 6.4
A double-blind, placebo-controlled, randomized phase III trial of gemcitabine plus bevacizumab versus gemcitabine plus placebo in patients with advanced pancreatic cancer: A preliminary analysis of CALGB 80303 Hedy Lee Kindler, Donna Niedzwiecki, Donna Hollis, Ebele Oraefo, Deborah Schrag, Herbert Hurwitz, Howard McLeod, Mary Mulcahy, Richard Schilsky, and Richard Goldberg for the Cancer and Leukemia Group B
CALGB 80303 Trial design R A N D O M I Z E Gemcitabine Bevacizumab Advanced pancreatic cancer N=590 Gemcitabine Placebo • Stratification: • Performance status: 0/1 vs. 2 • Extent of disease: metastatic vs. locally advanced • Prior radiation: yes/no
CALGB 80303: Overall Survival by Treatment Arm Bevacizumab 5.8 moPlacebo 6.1 mo HR = 1.03 P = 0.78
Phase III Study Comparing Gemcitabine plus Cetuximab versus Gemcitabine in Patients with Locally Advanced or Metastatic Pancreatic AdenocarcinomaSouthwest Oncology Group Protocol S0205 PA Philip, J Benedetti, C Fenoglio-Preiser, M Zalupski, H Lenz, B Goldman, E O’Reilly, R Wong, J Atkins, J Abbruzzese, C Blanke On behalf of SWOG, CALGB, NCIC, and the CTSU
S0205 Study Schema Gemcitabine + Cetuximab • Stratify • Locally advanced versus metastatic • Prior pancreatectomy • Yes versus No • Performance status • 0/1 versus 2 R A N D O M I Z E Gemcitabine
5.9 6.4 S0205: Primary EndpointSurvival of All Patients HR = 1.09 (95% CI: 0.93, 1.27)
ASCO 07, June 3rd. How to move on ? 1- Better knowledege on : pancreatic cancer cells relationships between tumoral, endothelial and stromal cells pancreatic cancer patients hopefully resulting in new drugs and new strategies 2- Optimize the available tools : Definitively separate strategies and studies in metastatic and in locally-advanced pancreatic cancer patients Prophylactic anticoagulation ? Gemcitabine-free regimens ?
#4519 Phase II trial of irinotecan/docetaxel for advanced pancreatic cancer with randomization between irinotecan/docetaxel and irinotecan/docetaxel plus C225, a monoclonal antibody to the epidermal growth factor receptor (EGF-r) : an Eastern Cooperative Oncology GroupStudy(E8200) B. A. Burtness, M. Powell, J. Berlin, D. Liles, A. Chapman, E. Mitchell, A. B. Benson, Eastern Cooperative Oncology Group Fox Chase Cancer Center, Philadelphia; Dana-Farber Cancer Institute, Boston; Vanderbilt University, Nashville; East Carolina University School of Medicine , Greenville; Thomas Jefferson University, Philadelphia; Northwestern University, Chicago
E8200 Study Design • Dexamethasone premedication • Docetaxel 35 mg/m2 followed by irinotecan 50 mg/m2 weekly x 4, q 6 weeks • Randomized phase II, 2 arms: • Irinotecan/docetaxel • Irinotecan/docetaxel + cetuximab loading dose of 400 mg/m2 followed by 250 mg/m2 weekly • All pts receive prophylactic enoxaparin if not on therapeutic anticoagulation
#4516 RANDOMIZED PHASE II TRIAL COMPARING FOLFIRINOX (5FU/LEUCOVORIN, IRINOTECAN AND OXALIPLATIN) VS GEMCITABINEAS FIRST-LINE TREATMENT FOR METASTATIC PANCREATIC ADENOCARCINOMAFIRST RESULTS OF THE ACCORD 11/0402 TRIAL M. Ychou1, F. Desseigne2, R. Guimbaud3, M. Ducreux4, O. Bouché5, Y. Bécouarn6, A. Adenis7, C. Montoto-Grillot8, E. Luporsi9, T. Conroy9 1. Centre Val d'Aurelle, Montpellier 2. Centre Léon Bérard, Lyon 3. Institut Claudius Regaud, Toulouse 4. Institut Gustave Roussy, Villejuif 5. Centre Hospitalier R. Debré, Reims 6. Institut Bergonié, Bordeaux 7. Centre Oscar Lambret, Lille 8. FNCLCC, Paris 9. Centre Alexis Vautrin, Nancy, FRANCE
Bolus 5-FU 400 mg/m2 2 h L-OHP 85 mg/m2 Leucovorin 400 mg/m2 Continuous 5-FU 2.400 mg/m2 CPT-11 180 mg/m2 2 h 46 h 1 h 30 Treatments Arm A : FOLFIRINOX (D1 = D14) Arm B : Gemcitabine (1000 mg/m² 30’ weekly 7 / 8, then 3 / 4 )
Results – Efficacy Investigators Response Rate* (ITT Population)
ASCO 07, June 3rd. How to move on ? 1- Better knowledege on : pancreatic cancer cells relationship between tumoral, endothelial and stroma cells pancreatic cancer patients hopefully resulting in new drugs and new strategies 2- Optimize the available tools : Definitively separate strategies and studies in metastatic and in locally-advanced pancreatic cancer patients Prophylactic anticoagulation ? Gemcitabine-free regimens ? Genomics and proteomics for individualized strategies ?
ASCO 07, June 3rd. #4521 K-ras mutation and EGF-r expression (Moore and coll, # 4521) Samples from 117 pts (out of the 569 included in the PA3 study) Only « trends » on survival, since sample size limits the conclusions. K-ras mutant (79% of pts) better than K-ras WT unexpected Among K-ras mutant : gem > or = to gem + T Among K-ras WT: gem + T > or = to gem expected expected Fish neg (53% of pts) better than Fish pos expected Among Fish pos, gem + T = gem Among Fish neg, gem + T > gem unexpected unexpected
Gem single agent still as standard treatment Bevacizumab EGF-r inhibitors Gem-free regimens Separate strategies for LA and M tumors Basic science New drugs Preclinical studies New early clinical trial designs Genomics, proteomics and individualized treatments ASCO 07, June 3rd. SUMMARY / TAKE HOME MESSAGES