RSV
RSV. RT 265. Respiratory Syncytial Virus. Manifests primarily as: Bronchiolitis Viral pneumonia Leading cause of lower respiratory tract infection in infants. Syncytium:. Multinucleate mass of protoplasm produced by the merging of neighboring cells. Incidence. Peak ages 2-8months


RSV
E N D
Presentation Transcript
RSV RT 265
Respiratory Syncytial Virus Manifests primarily as: • Bronchiolitis • Viral pneumonia Leading cause of lower respiratory tract infection in infants
Syncytium: Multinucleate mass of protoplasm produced by the merging of neighboring cells
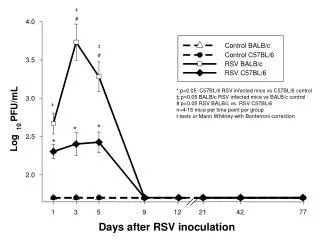
Incidence • Peak ages 2-8months • Usually >4years old • Mid-winter and spring months • Virtually all children have been exposed by 3rd birthday • Disease is mild in older children and adults (upper respiratory tract) • WHY THE LITTLE ONES? • Smaller airways • Reduced immune system • High-risk groups for severe RSV infection include the following: • premature infants in their first year of life (the younger the child is [gestational and chronological age] at the start of RSV season, the greater the risk) • Infants with chronic lung disease (eg, bronchopulmonary dysplasia,cystic fibrosis) during their first 2 years of life • Children with hemodynamically significant congenital heart disease, especially with increased pulmonary blood flow • Immunodeficient states • Children with metabolic and neuromuscular disorders • Children of multiple births (triplets or greater)
Diagnosis • Correlate symptoms with the time of year, presence of a regional outbreak, patient age, and history of the illness • Specific diagnostics testing: • Nasal swabs • Nasal lavage • Nasopharyngeal aspiration • CXR hyperinflation diffuse increase in interstitial markings
Presentation • Fever • Cough • Tachypnea • Retractions • Wheezing • Crackles • Sepsis like symptoms • Apneic episodes in the very young • Diffuse small airway disease
Management Supportive care Can be managed at home unless requiring: • Supplemental oxygen • Fluid replacement – normal feeding or IV if unable • Bronchial hygiene - suctioning • Bronchodilators? (alpha and beta agonists) • Ribavirin (Virazole) • Mechanical ventilation/CPAP Prevention • WASH YOUR HANDS • Avoid mucus membrane exposure • Palivizumab (Synagis) antiviral immunoglobulins /motavizumab (investigational – not FDA approved)
The “best” part: No lifelong immunity develops! Reinfection is common