Download
1 / 15
150 likes | 308 Views
Update on Study to Further Define the Incidence of T. cruzi Infection in the US Blood Donor Population. Susan L. Stramer, PhD American Red Cross BPAC Dec 15, 2010. Methods. The Ortho T. cruzi ELISA is used for donor screening

E N D
Update on Study to Further Define the Incidence of T. cruzi Infection in the US Blood Donor Population Susan L. Stramer, PhD American Red Cross BPAC Dec 15, 2010
Methods • The Ortho T. cruzi ELISA is used for donor screening • Repeat reactive (RR) donations are further tested using a research RIPA (Quest Diagnostics) • RIPA-pos donations are considered confirmed • Donors of RR donations are followed and tested by repeat serologic/parasitologic tests (hemoculture and PCR) • Donors are also asked to respond to a detailed survey regarding risk factors • For demographic/risk comparisons, RIPA-pos donors are defined as cases and RIPA-unconfirmed as controls
Methods • Following the implementation of selective testing, blood regions having the highest prevalence in the Southern portion of the US remained testing each donation (universal testing) to determine donor incidence • 3 ARC = SoCal (LA), TX and AR + CBCF (S FL) started 7/29/09 • 1 UBS site – Central Coast (CA) started 4/1/10
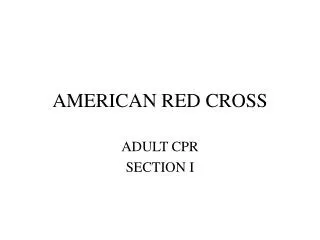
T. cruzi Reactive Donors by State of Residence (1/29/07–8/31/10) 3 1 2 5 5 5 109 1 5 1 5 16 4 DC 6 17 1 5 1 7 21 2 15 63 1 9 421 4 5 22 5 7 4 12 20 3 PR 14 2 5 7 7 43 220 28.1 million donations screened Overall: 1:25,100
ARC Risk Factors/Demographics to 8/31/2010 Univariate Analysis of 817 Completed Questionnaires Other variables with OR>1; p<0.05 = female gender, visited doctor after positive T. cruzi test result
Multivariate Analysisusing Step-wise Linear Regression of all ARC T. cruzi Donors who completed the Questionnaire 817 donors of 216/604 (36%) RIPA Pos (cases) and 602/1930 RIPA (31%) Neg/Ind (controls) to 8/31/10
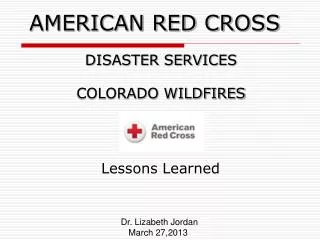
Documented Vector & Infected Reservoir in the US 56 Donors (48 ARC and 8 UBS) Investigated 15 Defined as Probable Vector and reservoir Vector only PR
Combined Lookback Experience * Two apheresis platelet recipients from two different donations from an Argentine PCR pos donor
Sensitivity of Various Testing Scenarios (22 month experience ARC) • Universal Testing (Ortho ELISA PI) • 860/861 = 99.88% (95% CI = 99.35% to 100.00%) • Born in an endemic area • 117/157 = 74.52% (95% CI = 67.83% to 81.87%) • Proportional difference of question to universal testing • 0.2472 (0.1738 to 0.3205); p<0.0001 • 1X screen negative to qualify donor • 378/394 = 95.94% (95% CI = 93.49% to 97.66%) • Proportional difference of 1X screen neg to universal testing • 0.0394 (0.0180 to 0.0609); p<0.0001
No Incident Cases Observed (22 month experience) • 2,482,904 ARC repeat donors with > 2 donations contributed 2,317,801 person years (pys) of observation • 1/29/07 – 11/30/08; 22-month experience • Only intervals between donations that were tested were counted • Mean interval = 0.934 years • 2,788,094 donors with > 2 donations contributed 2,585,134 pys when combined with UBS data • Included in the above: 13,680 UBS donors who indicated travel to Latin America since their prior test-negative donation • Limited time spent in endemic area
Incidence Study Protocol • Continue universal testing for 5 years to extend the timeframes for detection of incident infection in repeat donors in regions with presumed increased travel to endemic areas and those with the greatest likelihood of autochthonous infection • Universal testing in highest prevalence regions based on assumption that high prevalence regions = highest risk of incident infection • Other regions implemented selective testing • Add 2 million pys (5 million pys total) and extend interdonation interval to a mean of 1.9 years • Incident case = seroconverter • Screen RR and RIPA pos with a prior donation donation having a low signal and who has serologic progression on follow up
ARC Results with Selective Testing • Since August 09 with the conversion to selective testing, a stable reduction in testing volume has occurred (70%) • ~ 1:42,000 prevalence in selective testing regions (predicted 1:86,000) • ~ 1:12,000 in sites remaining on universal testing (predicted 1:6000) • No incident donors have yet been identified in ~ 4.6 million pys • 8 confirmed pos repeat donors in selective testing regions; 1 false-positive donor; 7 no prior T. cruzi test result • 18 confirmed pos repeat donors in universal testing regions; 3 false-positive donors; 15 no prior T. cruzi test result
43-month ARC Incidence Study Results • Isolated all donors that had screening performed regardless of test result (1/27/07-8/31/10); cumulative for all regions • 3,457,929 donors > 2 donations contributed 4,608,468 pys • Counted the interval in days between first and last screen to give person days/365 to give person years • Mean interval 487 days (1.33 years) • No seroconverting cases = 0 per 100,000 pys • Upper 95% confidence = 3.69 per 4,608,468 or 0.0801 cases per 100,000 pys • Less than 1 case per million pys • Criterion established for study: Upper limit of acceptable risk = 2.4 cases per million pys to be comparable with other infectious disease risks or 1-2 per year
Conclusions • A selective testing strategy based on qualifying a donor by a single negative donation has a high sensitivity and has significantly reduced the amount of testing required without compromising recipient safety