Download
1 / 67
670 likes | 863 Views
Lessons from Hypertension guidelines :. Treatment Of Hypertension. BY PROF.DR . KAMAL MAHMOUD AHMAD. HEAD OF THE CARDIOLGY UNIT MEDICAL RESEARCH INSTITUTE ALEX. UNIVERSITY. Easy to diagnose OFTEN remains undetected Simple to treat OFTEN remains untreated

E N D
Lessons from Hypertension guidelines : Treatment Of Hypertension
BY PROF.DR. KAMAL MAHMOUD AHMAD
HEAD OF THE CARDIOLGY UNIT MEDICAL RESEARCH INSTITUTE ALEX. UNIVERSITY
Easy to diagnose OFTEN remains undetected Simple to treat OFTEN remains untreated Despite availability of potent drugs, treatment is too OFTEN ineffective Hypertension even today is a triple paradox which is:
Guidelines • European Society of Hypertension • European Society of Cardiology • JNC 7 • Canadian Guidelines • Egyptian Guidelines
Relationship of Hypertensionto Its Comorbidities Rosamond W, et al. Circulation. 2007;115:69-171;
· Hypertension is a major health problem in Egypt with a prevalence rate of 26.3% among the adult population (> 25 years) . Its prevalence increases with aging, pproximately 50% of Egyptians above the age of 60 years suffer from hypertension. . MAGNITUDE OF THE PROBLEM IN EGYPT
EgyptianHTN Physician & Patient Survey* 1940 patients *M. Mohsen Ibrahim -
Poor understanding of the magnitude of the risk. Poor communication (doctor-patient) Patient forgetfulness. Lack of motivation. Logistic barrier ..Cost. Side effects. Complex regimen. Poor follow up. Causes of Discontinuation of The Drugs
Appropriate BP measurement 2008 • Allow the patients to relax for several minutes • Take at leasttwo measurements spaced by 1-2 min and additional measurements if the first two are quite different [use phase I and V (disappearance) Korotkoff sounds to identify SBP and DBP] • Use a standard bladder but have a larger for fat arms and a smaller one for thin arms and children • Have the cuff at the heart level • Measure BP in both arms at first visit to detect possible differences due to peripheral vascular disease. In this instance, take the higher value as the reference one • Measure BP 1 and 5 min after assumption of the standing position in elderly subjects, diabetic patients and in other conditions in which postural hypotension may be frequent or suspected (e.g. heart, renal failure, SNS dysfunction, use of vasodilative agents)
Home BP measurements • Self-measurement of BP at home should be encouraged • Response to antihypertensive therapy • Improving adherence with therapy • Evaluating white-coat HTN • On the contrary, Self-measurement of BP should be discouraged when: • it causes anxiety to the patient • it induces self-modification of the treatment regimen
Ambulatory BP Monitoring • ABPM is warranted for evaluation of “white-coat” HTN in the absence of target organ injury. • Ambulatory BP values are usually lower than clinic readings. • Awake, individuals with hypertension have an average BP of >135/85 mmHg and during sleep >120/75 mmHg. • BP drops by 10 to 20% during the night; if not, signals possible increased risk for cardiovascular events.
24-Hour Blood Pressure (n = 19)
Physical examination for secondary hypertension Signs suggesting secondary hypertension Features of Cushing syndrome Skin stigmata of neurofibromatosis (phaeochromocytoma) Palpation of enlarged kidneys (polycystic kidneys) Auscultation of abdominal murmurs (renovascular hypertension) Auscultation of precordial or chest murmurs; Diminished and delayed femoral pulses femoral BP (aortic coarctation or aorticdisease)
Laboratory Tests • Routine Tests • Electrocardiogram • Urinalysis • Blood glucose, and hematocrit • Serum potassium, creatinine, or the corresponding estimated GFR, and calcium • Lipid profile, after 9- to 12-hour fast, that includes high-density and low-density lipoprotein cholesterol, and triglycerides • Optional tests • Measurement of urinary albumin excretion or albumin/creatinine ratio • More extensive testing for identifiable causes is not generally indicated unless BP control is not achieved
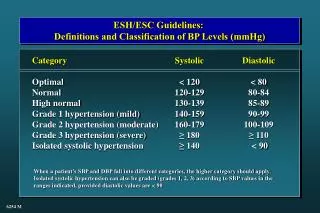
Blood pressure target values for treatment of hypertension II. Goals of Therapy
Lifestyle Recommendations for Prevention and Treatment of Hypertension
To reduce the possibility of becoming hypertensive, Reduce sodium intake to less than 2300 mg / day Healthy diet:high in fresh fruits, vegetables, low fat dairy products, dietary and soluble fiber, whole grains and protein from plant sources, low in saturated fat, cholesterol and salt in accordance with Canada's Guide to Healthy Eating. Regular physical activity:accumulation of 30-60 minutes of moderate intensity cardiorespiratory activity (e.g. a brisk walk) 4-7/week in addition to routine activities of daily living Maintenance of ideal body weight (BMI 18.5-24.9 kg/m2) Waist Circumference Men Women - Europid, Sub-Saharan African, Middle Eastern <94 cm <80 cm - South Asian, Chinese <90 cm <80 cm - Japanese <85 cm <90 cm Smoke free environment
Waist Circumference Measurement Last rib margin Mid distance Iliac crest Courtesy J.P. Després 2006
Lifestyle Recommendations for Hypertension: Dietary Dietary Sodium Less than 2300mg / day (Most of the salt in food is hidden and comes from processed food) Dietary Potassium If required, daily dietary intake >80 mmol Calcium supplementation No conclusive studies for hypertension Magnesium supplementation No conclusive studies for hypertension • • High in fresh fruits • • High in vegetables • • High in low fat dairy products • High in dietary and soluble fibre • High in plant protein • • Low in saturated fat and cholesterol • Low in sodium http://www.hc-sc.gc.ca/hpfb-dgpsa/onpp-bppn/food_guide_rainbow_e.html
Recommendations for daily salt intake Less than: 2,300 mg sodium (Na) 100 mmol sodium (Na) 5,8 g of salt (NaCl) 1 teaspoon of table salt 2,300 mg sodium = 1 level teaspoon of table salt
Lifestyle Recommendations for Hypertension: Physical Activity F I Intensity - Moderate T Time - 30-60 minutes T Should be prescribed to reduce blood pressure Frequency - Four to seven days per week Type cardiorespiratory activity - Walking, jogging - Cycling - Non-competitive swimming Exercise should be prescribed as adjunctive to pharmacological therapy
2007 ESC Guidelines for the management of arterial hypertensionConditions favouring use of some antihypertensive drugs versus others
Compelling and possible contraindications to use of antihypertensive drugs
Drug Treatmentyounger than 55 Step 1 : ACE inhibitor Step 2 : ACE inhibitor + Thiazide Diuretic or ACE inhibitor + Calcium Channel Blocker Step 3: A + C +D Step 4: Further diuretic therapy, alpha or B-blocker. If ACE inhibitor intolerant use A2RB
55 years or older or Black patients of any age Step 1 : C or D Step 2 : C + A or D + A Step 3 : A + C + D Step 4 : Add further diuretic therapy or alpha or beta blocker If ACE inhibitor intolerant use A2RB
2008 Canadian Hypertension Education Program (CHEP) Table of contents Indications for drug therapy Goal for therapy Adherence Lifestyle Uncomplicated CV – IHD CHF Cerebrovascular / Stroke LVH X. Chronic kidney disease Renovascular Diabetes Smoking Global risk reduction
V. Choice of Pharmacological Treatment Uncomplicated NO YES Treatment in the absence of specific indication Individualized Treatment (and compelling indications) Associated risk factors? or Target organ damage/complications? or Concomitant diseases/conditions?
Treatment of Adults with Systolic/Diastolic Hypertension without Other Compelling Indications ARB ACE-I TARGET <140/90 mmHg INITIAL TREATMENT AND MONOTHERAPY Lifestyle modification therapy A combination of 2 first line drugs may be considered as initial therapy if the blood pressure is >20 mmHg systolic or >10 mmHg diastolic above target Thiazide Long-acting CCB Beta-blocker* * BBs are not indicated as first line therapy for age 60 and above ACEI and ARB are contraindicated in pregnancy and caution is required in prescribing to women of child bearing potential
Add-on Therapy for Systolic/Diastolic Hypertension without Other Compelling Indications 1. Add-on Therapy • CONSIDER • Nonadherence? • Secondary HTN? • Interfering drugs or lifestyle? • White coat effect? 2. Triple or Quadruple Therapy If partial response to monotherapy If blood pressure is still not controlled, or there are adverse effects, other classes of antihypertensive drugs may be combined (such as alpha blockers or centrally acting agents).
Treatment of Systolic-Diastolic Hypertension without Other Compelling Indications Long-acting CCB Beta-blocker* Thiazide diuretic ACE-I ARB TARGET <140/90 mmHg Lifestyle modification A combination of 2 first line drugs may be considered as initial therapy if the blood pressure is >20 mmHg systolic or >10 mmHg diastolic above target Initial therapy Dual Combination • CONSIDER • Nonadherence? • Secondary HTN? • Interfering drugs or lifestyle? • White coat effect? *Not indicated as first line therapy over 60 y Triple or Quadruple Therapy
ESH & ESC 2007 GuidelinesPossible combinations between some classes of antihypertensive drugs Thiazide diuretics Angiotensin receptor antagonists β-blockers Calcium antagonists α- blockers ACE inhibitors The preferred combinations in the general hypertensive population are represented as thick lines.
New components and functions of the (RAS) system Since then, an expanded view of RAS has gradually emerged. Local tissue RAS systems have been identified in most organs. Evidence for an intracellular RAS has been reported. The new expanded view of RAS therefore covers both endocrine, paracrine and intracrine functions.