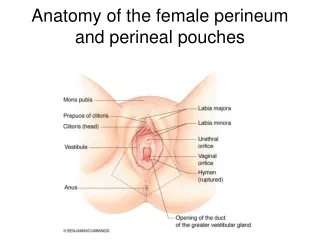
Complex Perineal Injuries
Complex Perineal Injuries. Dr. Bennet Rajmohan, MRCS(Eng), MRCS(Ed) Consultant General Surgeon. Case Study. 27 yrs / male Hit by lorry, 1.30pm, Mar 2011. Brought to A&E by 1.55 pm Profuse bleed from left thigh & perineal wound O/E – HR 98 / min, BP not recordable, GCS – 15 / 15

Complex Perineal Injuries
E N D
Presentation Transcript
Complex Perineal Injuries Dr. Bennet Rajmohan, MRCS(Eng), MRCS(Ed) Consultant General Surgeon
Case Study • 27 yrs / male • Hit by lorry, 1.30pm, Mar 2011. Brought to A&E by 1.55 pm • Profuse bleed from left thigh & perineal wound • O/E – HR 98 / min, BP not recordable, GCS – 15 / 15 • Chest, pelvis, long bones, abdomen – normal
Case Study • Resuscitated • Ultrasound abdomen – Solid organs normal, no haemoperitoneum • X-rays – fracture left lateral malleolus • Advised wound debridement and colostomy • CT chest & abdomen – Extensive degloving injury left groin, perineum & thigh. No pelvic fracture. Abdomen – normal
Surgery 1 • Delays, some avoidable • A&E ICU OT …….> 6hours • BP dropped to 70mmHg on anaesthetic induction Dopamine started • Surgery 1 – Wound debridement & compression bandage, not stable enough for colostomy. Post-op BP – 70 / 40 • ICU elective ventilation, Dopamine
Surgery 2 • POD 1 – Extubated. POD 2 – Off Dopamine, increasing swelling of left leg, ? Compartment syndrome • POD 3 – Surgery 2 – Dressing change, overall healthy appearing wound skin graft to groin, fasciotomy left leg • Colostomy deferred again, as deemed not fit for a further 2-hour surgery
The Tsunami… • POD 3 – 6 fever with chills, massive sepsis, confusion, aggressiveness • POD 7 – HR 160 / min, raging fever • Perineal wound swab – Pseudomonas sensitive to Imipenem only, antibiotics escalated • Surgery 3 ORIF ankle, defunctioning sigmoid colostomy & extensive wound debridement groin & thigh
….........Finally • POD 9, 11,13 – Serial debridement in ICU under IV sedation. Fever settled. Stoma healthy & working well • Femoral line – Pseudomonas. Ankle & colostomy site wound infections • POD 15 – Surgery 4 Debridement & extensive skin grafting. Dopamine for 2 days • 4 further dressings in ICU, discharged on day 27, graft take about 70%
Follow-up • Weekly dressings in EOT, further graft loss • Surgery 5 Further debridement & skin grafting 4 months later • Eventual complete healing, but…..Donor site infection(right thigh), requiring weekly dressings • 9 months after injury – Surgery 6 colostomy closure & skin graft donor site
Discussion Complex perineal injuries • Exsanguination within few hours • Among survivors, high risk of wound sepsis / septicaemia – 70 – 80 % • Combination of 1) Inadequate debridement of necrotic tissue 2) residual haematoma and 3) faecal contamination deadly!!
Discussion • World Journal Of Surgery, 2003. University of Wisconsin Hospital, Wisconsin, USA Management principles • Resuscitation, haemorrhage control – avoid femoral lines • Definition of associated injuries – limited X-rays (Chest, C-spine, pelvis), avoid or defer CT • Early stabilisation of pelvis in A&E, if necessary • Aggressive soft tissue debridement & pulsatile irrigation • Faecal diversion with distal rectal wash, urinary diversion or BOTH, within 48 hrs
Discussion Management principles(contd) • Enteral access (feeding jejunostomy) & early enteral feeding • Mandatory daily sharp debridement & pulsatile irrigation, at least for 3 to 4 days • Fixation of other fractures • Eventual soft tissue coverage with skin grafts or flaps or both • IVC filter placement to prevent fatal pulmonary emboli
Fast-track Surgery Dr. Bennet Rajmohan, MRCS(Eng), MRCS (Ed) Consultant General Surgeon & Dr. Abdul Khader, MD Consultant Anaesthetist
Sigmoid Colostomy Closure Day1 – planned admission after pre-op counselling • Soft diet, plenty of liquids orally • No PEGLEC bowel preparation, no IV fluids • 700 ml high-carb drink over 1 hour, evening before surgery • Syr. Lactulose 15 ml bd, Zolfresh Day 2 – day of surgery • Liquids upto 2 hrs before surgery, including 300 ml high-carb drink , Syr. Lactulose, Perinorm, PPI • Epidural analgesia + IV anaesthetic agents • Antibiotic prophylaxis
Day 2 (contd) • Skin graft right thigh and Oblique left iliac fossa incision end to end single layer sigmoid anastomosis • No drain, no nasogastric tube • “Dry regimen” – intra-op IV fluid < 2litres • Warmer & warmed IV fluids • Short acting opiates, NSAIDs • Post-op ward, post-op Heparin • Chewing gum, toffees, liquids started 2 hours post-op
Day 3 (POD 1) • Epidural analgesia, no IV or IM or oral opiates • Foley catheter removed @ 6 am – voided • Soft diet started, passed flatus, stools 3 times • Antibiotics, IV fluids stopped • Mobilisation 6hrs, Shifted to ward Day 4 (POD 2) • Mobile, climbing up stairs. Normal diet • Epidural catheter removed • Discharged by 1pm (< 48 hrs post-op)
Outpatient review POD 5 • SSG dressing change – graft take 100% • Colostomy closure wound clean POD 12 • SSG dressing – clips removed • Abdominal sutures removed POD 19 • Wound clean, SSG take 95%
Fast-track Surgery • Multimodal rehabilitation or Enhanced recovery after surgery (ERAS) • Professor Henrik Kehlet , a GI surgeon, Copenhagen University, Denmark • Planned discharge after 48hrs in patients undergoing elective open colonic surgery for malignant & benign diseases
The Concept • Comprehensive evidence-based program • Improves post-operative recovery by reducing stress related organ dysfunction • Discharge criteria (mobile patient, pain-free on oral analgesics, fully recovered bladder & bowel functions) are same BUT achieved earlier
Preoperative Period • Stabilise coexisting diseases, encourage ‘prehabilitation’ program, stop smoking (2mths) & alcohol (4wks), optimise DM / HT / chest etc • Minimise patient anxiety, counselling • Ensure adequate hydration & nutritional support, modern fasting guidelines, no bowel preparation • Prophylaxis to prevent post-op complications (eg., nausea, vomiting, pain, ileus)
Intraoperative Period • Anaesthetic agents / techniques which allow optimal surgery, with rapid recovery & minimal side-effects • Local anaesthesia – blocks, wound infiltration, instillation • Pre-emptive & multimodal analgesia , antiemetic prophylaxis • Avoid hypothermia & excessive fluid administration • Minimise use of nasogastric tubes & drains
Postoperative Period • Ensure adequate pain control with epidural & non-opioid analgesics. Minimise opioids • Early ambulation • Early enteral feeding, even in case of some anastomoses • Early discharge
The Results • hospital stay • No morbidity • No readmission • No safety • patient satisfaction • cost • Earlier ambulation • muscle function • oral intake • loss of lean mass, fatigue • pulmonary function • Earlier GI motility • exercise capacity, cardiovascular function
Retrospective • Colonic resection • Stomas excluded • LAR excluded • Acute surgeries excluded • Two hospitals • Conventional care (130 patients) • With “multimodal rehabilitation” (130 patients) Basse et al. Colonic surgery with accelerated rehabilitation or conventional care. Dis Colon Rectum. 47: 271-278, 2004.
130 patients in each group All figures significant Basse et al. Colonic surgery with accelerated rehabilitation or conventional care. Dis Colon Rectum. 47: 271-278, 2004.
Basse et al. Colonic surgery with accelerated rehabilitation or conventional care. Dis Colon Rectum. 47: 271-278, 2004.
Fast-track surgery Summary
Take-home Messages • Complex perineal injuries – No room for a “softly-softly” or “ wait and see” approach • Rethink conventional peri-operative care, fast-track surgery beneficial & safe • In all affairs, it's a healthy thing, now and then to hang a question mark on the things you have long taken for granted - Bertrand Russell, British author, mathematician & philosopher (1872 - 1970)