Download
1 / 37
400 likes | 578 Views
Assessing study quality for a systematic review. Trudy Bekkering , PhD Center of Evidence-Based Medicine & Belgian Branch of the Dutch Cochrane Center Centre for Methodology of Educational Research Katholieke Universiteit Leuven, Belgium. Why is it so important?.

E N D
Assessing study quality for a systematic review Trudy Bekkering, PhD Center of Evidence-Based Medicine & Belgian Branch of the Dutch Cochrane Center Centre for Methodology of Educational Research KatholiekeUniversiteit Leuven, Belgium
Why is it so important? • Meta-analysis aims to increase precision • Meta-analysis of studies with bias in results gives very precise but wrong results • Garbage in, garbage out
Bias versus imprecision Bias: • A systematic error in the results or the inferences • Methodologicalflaw • Overestimation or underestimation
Bias versus imprecision BIAS Idealstudy
Bias versus imprecision Imprecision: • A random error in the results • Sample variation • Direction of error is random
Bias versus imprecision IMPRECISION Ideal study
Bias versus imprecision BIAS + IMPRECISION
Bias versus imprecision BIAS ? IMPRECISION?
Risk of bias versus bias • Clearempiricalevidencethatparticularflaws in study design can lead to bias. • Usuallyimpossibletoknowtowhatextentbiaseshave affected the results. • Keyconsideration = should the resultsbebelieved
Tools for assessing study quality Scales: discouraged Checklist: between 3 and 57 items Cochrane tool: “domain based” Depends on study design
Tool for RCTs: Cochrane tool Risk of bias on 6 domaines: • Sequencegeneration • Allocationconcealment • Blinding • Incomplete outcome data • Selectivereporting • Other sources of bias
Blinding of intervention • Participants (patients, clients) • Care providers (doctors, nurses, teachers …) • Outcome assessors
Incomplete outcome data “Attrition” (drop-out): no data • Withdrawal • Do notattend follow-up appointment • Failure to complete questionnaire / diaries • Cannotbelocated (lost to follow-up) • Decisionby investigator tocease follow-up • Data or records are lost
Incomplete outcome data “Exclusion”: data available, but excluded from analysis • Participants found to be ineligible after enrolment • An “as treated” (or per-protocol) analysis:participants are only included if they received the intended intervention in accordance with the protocol
Selectiveoutcomereporting • = selection of a subset of the variables recorded for inclusion in publication, • on the basis of the results • For example: • Omission of non-significant outcomes • Choice of data for an outcome (e.g. osteoporosis) • Choice of analysis (e.g. blood pressure) • Reporting of subsets of data (e.g. sepsis) • Under-reporting of data (e.g. only “not significant”)
Presentation in your review “Risk of bias graph”
Assessing risk of bias in NRS • Selection bias (how was groupallocation?) • Performance bias (blinding, fidelity of interventions) • Attrition bias (completeness of sample & follow-up) • Reporting bias (selectiveoutcomereporting) • Confoundingandadjustment
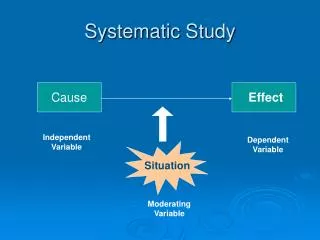
Confounding ? ? Imbalance in prognostic factors Comparison intervention - control Intervention versus control Difference in outcome
Confounding Confounding factor Association between 2 factors Presence of risk factor Occurrence of outcome
Confounding & adjustment • At the stage of protocol: list potential confounding factors • Identify the factors the authors have considered and omitted • Assess balance between groups at baseline • What did authors do to control for confounders (matching, restricting to subgroups, stratification, regression modelling)
Tool for NRS Downs and Black instrument (J Epidemiol Community Health 1998;52:377-84) 27 items: • Reporting (10) • Externalvalidity (applicability) (3) • Internalvalidity - bias (7) • Internalvalidity – confounding (6) • Power (1)
Downs and Black instrumenthttp://www.nccmt.ca/ registry/view/eng/9.html
Tool for NRS Newcastle-Ottawa Scale (NOS) (Wells 2008) 8 items covering 3 perspectives: • Selection of studygroups • Comparibility of groups • Ascertainement of exposure (case-control) or outcome (cohort)
http://www.ohri.ca/programs/ clinical_epidemiology/oxford.asp
Diagnostic studies QUADAS tool Whiting BMC Medical Research Methodology 2003;3:25 Cochrane version: 11 items (out of 14 original) Diagnostic Test Accuracy Working Group: handbook http://srdta.cochrane.org/ handbook-dta-reviews
Other risk of bias assessment tools SIGN (Scottish Intercollegiate Guidelines Network) http://www.sign.ac.uk/methodology/ checklists.html
In summary • Risk of bias assessment is essential for systematic reviews • For RCT: use the Cochranetool • For NRS: • Higher risk of bias (selection bias & reporting bias) • Use the appropriate tool toassess risk of bias • Considerhowpotentialconfounders are addressed