Download
1 / 12
120 likes | 136 Views
Learn about the principles and history of clinical governance, service user involvement, and the importance of quality in healthcare. Explore how to effectively use clinical information and NICE guidance.

E N D
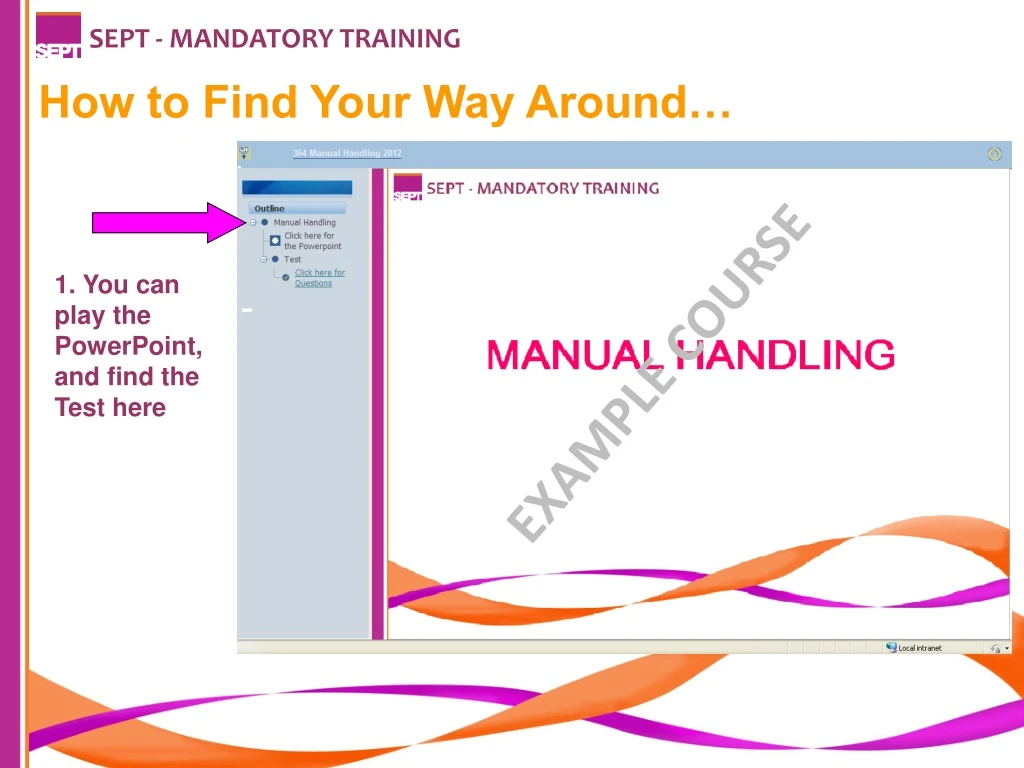
SEPT - MANDATORY TRAINING How to Find Your Way Around… 1. You can play the PowerPoint, and find the Test here EXAMPLE COURSE
SEPT - MANDATORY TRAINING 2. You can minimise this column and make the main page bigger by clicking this icon. Click it again to bring it back. EXAMPLE COURSE
SEPT - MANDATORY TRAINING 3. Always click this ‘Home’ icon to save your progress and log off. This is very important! EXAMPLE COURSE
SEPT - MANDATORY TRAINING Clinical Governance What is Clinical Governance? Clinical Governance is about providing a patient-centred, accountable, safe and high quality service in an open and questioning environment. Clinical Governance questions traditional structures and ways of doing things and creates a consistent and sustained approach to improving the quality of healthcare. COURSE OBJECTIVES • What Clinical Governance is; • History of Clinical Governance; • Service User involvement; • PALS involvement; • Use of clinical information; • NICE guidance; • Useful contacts. Definition of Clinical Governance “A framework through which NHS organisations are accountable for continuously improving the quality of their services and safeguarding high standards of care by creating an environment in which excellence in clinical care will flourish".
SEPT - MANDATORY TRAINING Definition of Quality There have been several definitions of quality care in the last 20 years The definition below was adopted by the NHS in 2008 Quality treatment and care has three elements which must come together to ensure the delivery of HIGH QUALITY CARE: Effectiveness of the treatment and care provided to patients – measured by clinical outcomes and patient related outcomes The Safety of treatment and care provided to patients The experience patients have of the treatment and care they receive (Lord Darzi, NHS Next Stage Review, Leading Local Change, May 2008.) The NHS Constitution (2010) enshrines the right of people to receive high quality care and treatment
SEPT - MANDATORY TRAINING History of Clinical Governance 1997 : Labour Government in the White Paper ‘The New NHS’ – Modern & Dependable abandoned the internal market and introduced a statutory duty for quality improvement that was called CLINICAL GOVERNANCE. 1999: Trust Boards assumed a legal responsibility for quality of care that is equal in measure to their other statutory duties. Clinical governance is the mechanism by which that responsibility is discharged 2003: This “Duty of Quality” is a legal requirement and is found in the Health and Social Care (Community Health and Standards) Act 2003: 2004: Health Commission established to improve the quality of services in the NHS 2009: Department of Health.: A First Class Service 2009: Standards for Better Health Declaration 2009: Care Quality Commission to regulate National Standards across health and social care providers
SEPT - MANDATORY TRAINING Service User Involvement The Legislative Framework to ‘put patients at the centre of care’ was announced through the NHS Plan -Section 11 of the Health and Social Care Act 2001; This act came into force on 1st January 2003 and states that all Trust’s must, as a matter of course, consult and involve patients and members of the public; Consult not just when a major change is proposed, but in the on going planning and development and the delivery of services day to day. • Key Components of Clinical Governance • Person centred care with service user involvement Visible Trust Board Level leadership • Use of Clinical Information; • Patient safety and robust risk management; • Clinical Audit; • Research & Development • Clinical Effectiveness • Staffing & Management; • Feedback from Service Users • We must actively seek feedback from our service users and make sure that action and changes occur in response to this feedback. Feedback can come from a variety of sources: • Sources of Feedback • Complaints / compliments; comment cards • National Surveys (including the National Patients Survey); • Local Surveys; • Advocacy services • The Patient Advice and Liaison Service (PALS); • Patient’s experience group (PEx). • Involvement in the annual Business Planning cycle along with staff and other stakeholder groups • Service user son recruitment panels • Staff induction training for staff • Take it to the Top Forums give direct access to the Chief Executive and Team • Mystery Shoppers • Focus Groups
SEPT - MANDATORY TRAINING Trust Board Leadership Regular visits from executive and non-executive directors to clinical areas to discuss element of quality and safety: Patient safety walk rounds Director CQC spot checks Improvement programmes led by directors and senior management. • PALS Involvement • Patients, relatives or carers may sometimes need help, advice or support; • PALS will provide confidential advice and support, helping with any concerns about the care provided by the Trust; • PALS can guide patients, relatives and carers through the different services available • Use of Clinical Information - Evidence • Clinical Governance requires evidence of effective patient care and safe and appropriate services; Accurate, meaningful and reliable information provides a vital support to quality improvement processes; • Information comes from many different sources including: • Routine monitoring and reports; • Clinical Audit; • Essence of Care Benchmarks • Productive Series outcomes • Patient & Carers surveys • Ward Dashboards
SEPT - MANDATORY TRAINING • Risk Management • People Safety is about ensuring that people in our care receive high quality care and treatment by the right people at the right time in the right place. • There are risks associated with all episodes of care. • Risk Management is about minimising risks to patients and staff; • It is a positive function and central to the quality of care we give to patients • Risks need to be avoided or controlled; • We do this by carrying out a Risk Assessment and agreeing the level of seriousness attached to each risk; • Actions are then taken on the result of the Risk Assessment to ensure everyone's safety. • Where risks cannot be completely removed we aim to minimise the harm caused by any adverse incidents. • Risk Management is about "stopping bad things from happening" • Clinical Audit • As part of local arrangements for clinical governance, all NHS organisations are required to have a comprehensive programme of quality improvement activity that includes clinicians participating fully in audit; • Clinical audit is the component of clinical governance that offers the greatest potential to assess the quality of care routinely provided for NHS users – audit should therefore be at the very heart of clinical governance systems; • National Institute for Health & Clinical Excellence (NICE). • Clinical Audit is part of the CQUIN and Quality Account work undertaken in local areas in partnership with commissioners
SEPT - MANDATORY TRAINING Research & Effectiveness - Evidence Based Practice The work that we carry out daily should be based on accepted good practice. It should be proven to be appropriate and effective by people with knowledge and expertise. This is evidence based practice; The guidance provided by the National Institute for Health & Clinical Excellence (NICE) is a good example of evidence based practice. NICE Guidance NICE develop and distribute guidelines, technology appraisals (Drugs and equipment) and quality standards on a national level. These guidelines are all evidence based and well researched before distribution. Each Trust within the country is responsible for evidencing compliance with the NICE Guidance. The Head of Clinical Effectiveness has responsibility to ensure that we are applying all the NICE guidelines, where appropriate. Local NICE Groups have responsibility to ensure that where guidance is applicable there is an achievable action plan in place monitored within the service and progress sis reported to the Clinical Effectiveness Group (CEG) The Clinical Effectiveness Group (CEG) is responsible for ensuring that key decisions are made in relation to NICE guidelines.
SEPT - MANDATORY TRAINING Doing things differently If you do what you always did, you get what you always got! • Staffing & Management • The Trust aims to: • have staff that are well trained and have appropriate skills to provide a high quality service through: Training; • Education; • Appraisal; • Clinical & Managerial Supervision • Education & Training • The Trust aims to: • Develop staff, at all levels, to their full potential, as a means of providing high quality, efficient and effective services and individual patient care; • Become a centre of excellence for lifelong learning which is fundamental to the continuous improvement of services to patients and to fulfilling the local and national objectives; • Supporting personal growth, career development and employability, against a background of ongoing organisational change. Care Quality Commission The purpose of the Care Quality Commission is to promote improvements in the quality of healthcare and public health, through independent, authoritative, patient-centred assessments, of the performance of those who provide services. From 1 April 2009 the Care Quality Commission brought together the Commission for Social Care Inspection, the Healthcare Commission and the MH Act Commission. All Trusts are monitored by the Care Quality Commission.
SEPT - MANDATORY TRAINING Now You need to take the Test. Please click the ‘Test’ icon in the left column, and then click for Questions. Remember to click the ‘Home’ icon when you finish the Test to save your results EXAMPLE COURSE















