Download
1 / 18
190 likes | 229 Views
Learn about the physiology, assessment findings, and nursing management of Hyperparathyroidism and Hypoparathyroidism. Explore collaborative treatments, including surgery and post-op care for both conditions.

E N D
Disturbances of the Parathyroid Ann MacLeod, RN, BScN, MPH
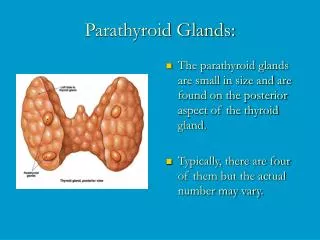
Objectives • Review anatomy and physiology of Parathyroid gland • Understand Hyper and Hypoparathyroid • assessment findings • nursing diagnoses • management
Hyperparathyroidism • Overactivity of one of the parathyroid gland • classified as primary or secondary • 90% caused by adenoma • 8% by hyperplasia or hypertrophy • 2% by carcinoma
Physiology • Normal function of PTH is to control and increase bone resorption of calcium, therefor maintain ca+ and phos. Ions within the bloodstream
Bone damage muscles become hypotonic fatigue, muscle weakness cardiac muscle may be affected with arrhythmias Back ache, joint pain fractures, deformities n/v, constipation large amts. Of calcium passing through the kidneys may cause kidney stones Assessment: excessive blood calcium causes: Hyperparathyroidism
Collaborative Treatment • Primary: always treated surgically (1/2 of one gland is sufficient to sustain the body • secondary: managed by correcting the cause
Para-thyroidectomy • Pre-op: while ct. awaits surgery: push fluids to > 3000mls/day, cranberry and prune juice prevents stone formation and decreases infection • low Ca+ diet; no milk or milk products • prevent constipation; increase activity, stool softeners, laxatives
Parathyroidectomy Pre-op care cont’d • Strain all urine; observe for hematuria and renal colic • protect from injury d/t path. #s • Phosphate or Sodium Phytate(Rencal) this drug decreases absorption of calcium in the gut • calcitonin: decreases serum calcium
Immed. Post.op observe for hemorrhage and airway obstruction watch for serious decrease in blood calcium which will produce tetany Tetany could be so severe and lead to muscle twitching and seizures Rx. IV calcium gluconate Hungry Bone Syndrome: Post-operative Care:
May need to increase calcium in the diet post. Op calcium gluconate injections Oral calcium preparations Post-op Parathyroidectomy cont’d
Hypoparathyroidism • Hyposecretion of PTH causes decreased blood calcium, and increased serum phosphorus • leads to pronounced neuromuscular irritability
Causes • Accidental removal of parathyroid gland • auto immune destruction • congenital absence of the glands
Tetany numbness and tingling of fingers painful muscle spasms chvostek’s sign: hyperirrritability of facial nerve Trousseau’s sign: carpal spasm of fingers and hand after pressure cuff deflated laryngeal spasm may also occur>>dyspnea severe : can affect cardiac muscle>heart failure Assessment: caused by low serum calcium levels
Hypoparathyroidism - Assessment Cont’d • Chronic: lethargy, brittle nails, constipation, loss of tooth enamel, muscle pains • diagnosis is made based on the presence of Chvostek’s and Trousseau’s sign and also decreased calcium
Collaborative Management • Acute: can be life threatening; • goals: increase calcium rapidly, prevent and or treat possible convulsions, and control laryngeal spasms and possible resp. obstruction
10% calcium gluconate by IV Trach set and ET tube while emergency in progress oral Calcium and Vit. D Diet: Increase ca+, calcium supplements Lifelong medication and follow-up blood work full recovery if diagnosed early Management