Download

1 / 31
430 likes | 700 Views
STAFF BRIEFING Care Quality Commission (CQC) Essential Standards of Quality and Safety. Preparing for inspection. STAFF BRIEFING. The purpose for this briefing is to: Help staff familiarise themselves with the new inspection model

E N D
STAFF BRIEFINGCare Quality Commission (CQC)Essential Standards of Quality and Safety Preparing for inspection
STAFF BRIEFING The purpose for this briefing is to: • Help staff familiarise themselves with the new inspection model • Explain how the CQC will inspect so that the actual visit feels less daunting • Shine a light on the areas of risk identified through our own quality inspections • Provide practical advice on how to prepare
The role of the Care Quality Commissioner: Independent regulator of all health and social care services in England • The independent regulator of all health and social care services in England • Care provider registration • Set National Essential Standards of Quality and Safety • Compliance monitoring and regulation of services against standards through: • Data and surveillance pre inspection and at regular times during the year • Direct observations and interviews at inspection • Action – where standards are not being met.
St George’s CQC inspection • The Care Quality Commission (CQC) inspection starts on Monday 10th February 2014 • It will last for one week but there could be shorter follow-up visits in the terms of unannounced inspections • Inspection will cover St George’s and Queen Mary’s Hospital and our community services • 40-50 inspectors divided in to 12 teams. Inspectors will be wearing colored id badges • Six teams will focus on St George’s and six will focus in the community • The inspectors will observe care in practice, also talk to staff, patients and our key stakeholders • A rating of ‘good’ or ‘outstanding’ is required for us to continue our path to becoming a Foundation Trust.
CQC Inspection model • Since our last inspection a new, more rigorous, inspection model has been devised by the Chief Inspector of Hospitals • The new regime and approach to inspections will be based around 5 key domains Four point scale used for all ratings • 5 inspection questions • Are they safe? • Are they effective? • Are they caring? • Are they well led? • Are they responsive • Outstanding • Good • Requires Improvement • Inadequate
NEW CQC INSPECTION REGIME Chief Inspector of Hospitals • Decisions on where and when to inspect will be made by using information in a more focused and open way, responding quickly to services that are failing • National and local data sources will continue to be used along with intelligence from local authority overview and scrutiny committees • A set of 118 indicators to provide information on each element of the new surveillance model. “Smoke detectors” by which they will decide where and when to inspect - which helps to develop their key lines of enquiry • Mortality data features highly in the proposed data set along with patient / public comments posted on various web sites.
CQC Inspection model During an inspection the CQC Inspectors will: • Hold focus groups with peoplewho use services(includingrelatives) about their experiences of receiving care • Hold small group meetings with leaders of key services • Hold focus groups with staff (multidisciplinary teams – including students) • Interview individual directors as well as staff of all levels • Observe patient care to check that the right systems and processes are in place, and patients are treated with kindness, dignity and respect and staff work well and communicate effectively with each other and patients • Look for evidence that care is meeting national standards • Look at documentation – have observations been done, medication given, risk assessments completed, plans of care • Observe staff interaction – are teams supportive and respectful of each other • Look at environment – is it clean, uncluttered and safe • Look at patient information available – are notice boards up to date, relevant, tidy.
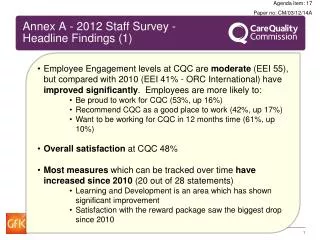
Promoting high-performance and excellence • The CQC revisit in August found a much improved position across the St George’s Hospital site • The majority of the patients they spoke said that they had a good experience at St George’s and were very positive about the care they received from staff • Don’t forget that these inspections are an opportunity for us to nationally showcase the quality and safety of care we provide • We continue to use each inspection as a driver for quality improvement. For example CQC inspections have now become quality inspections and form part of our internal assurance processes to check that we are consistently achieving good standards of care.
Advice from a senior nurse It’s about flexibility because what may be important during one inspection may not be an issue at another… It’s important to remember that getting the little things right quickly accumulates into getting the big things right. It’s also worth remembering the opposite is true… Ensure all members of staff are aware of the identified areas of concern and all members of staff have a ‘voice’… Be prepared, be receptive to change and learn from any shortcomings the inspectors might raise… It’s important not to take things personally or think inspectors are nit-picking. You need to listen to what they have to say, address any issues raised…
If you speak to an inspector • Maintain a professional manner at all times. There is no such thing as a ‘throw away’ comment • Think carefully about how you speak about yourself, your colleagues and your environment. Always talk about colleagues and services in a professional manner • Listen to what is being asked – ask for clarification if need be. Think about your reply. It’s ok to pause to collect your thoughts • If you aren’t certain how to respond to a question or feel compromised by any line of questioning, or if you can’t answer a question, say so but also say that you will find out. • As well as being asked about what you do or what you know you may be asked about things that concern you. It is absolutely right that you are open and honest. Try to balance your concerns with information about what is being done. • Think about the positive effects your care provides to families and patients who you work with on a day-to-day basis and over the long-term. • Remember, if you make a comment about the service, inspectors may check the validity of what you said against other evidence.
Tips for working under inspection It is a fact of life that people act/work differently whilst being observed. The following points are suggestions to help you whilst working under observation • Don’t get paralysed by perfection • Be yourself, and use the inspection to showcase your work • Stay in the moment?- if you feel overwhelmed (like pretty much everyone) it might not be because you have so much to do rather you trying to do so much at the same time. • Keep calm • Even though you may feel you are being watched always consider the patient needs first
Are we safe?: CQC Key Lines of Enquiry What does this mean in your daily practice?
What does this mean in your daily practice POLICES AND PROCDURES • Mental Capacity Act • Independent Mental CA • Safeguarding Adults • Safeguarding Children • Infection Prevention and Control • Medicine Safety • Monitoring Drug and Fridge Temperatures • Health and Safety • Waste Management • Medical Equipment • Safe Staffing Available via the intranet homepage PRACTICAL APPLICATION Complaints posters Learning from incidents Audits - Results and where to improve ID bands in place IC - Hand gel & hand washing/ equipment Sluice - clean and tidy Call bells near patient Clutter free ward - Dump the junk Handling linen Safe surgery checklist Patient surveys
What can you do prior to inspection • Consider the following questions: • Do I report/act on concerns about unsafe equipment? • Do I know how to report a safety incident? • Do I always wash my hands or use hand gel between patients? • Do I follow Trust policies in relation to medication? • Do I know how to resolve or advise a patient who has concerns? • Do I ensure written and electronic patient information is kept secure? • Do I keep the information available to patients up to date? • Do I observe the dress code or uniform policy including bare below elbows • Do encourage patients to provide feedback on our services? • Do I complete all appropriate risk and document assessments ? • Do you assess your patient acuity / dependency at handover and ensure you have sufficient staff to cover the required work for the shift • Do I know the procedure to follow for a patient who might have a lack of mental capacity? • Do I provide bank, temporary, agency or junior staff with adequate support at the start of a shift?
Quality Inspections: Identified Safety Risks • Not all staff are aware of how access an interpreter. • Cleaning & Decontamination green labels are not always on equipment to identify it has been cleaned. • Not all staff have completed 'Basic Awareness of Safeguarding Vulnerable Adults and Adult Protection', which is part of mandatory training for all staff working within the Trust. • The target of 96% of VTE risk assessments to be fully completed within 24 hours of admission has not been delivered in Quarter 2. Certain divisions have performed poorly, dropping from a completion rate of 70% to 53% • The outcome of the WHO Checklist Compliance has shown poor compliance rate for Briefing and Debriefing and the common reasons documented were “the team do not do the debriefing regularly”,
Are we effective ? CQC Key Lines of Enquiry What does this mean in your daily practice?
What does this mean in your daily practice? POLICIES AND PROCEDURES • Information Governance • Consent • Records Management • Accessing Policies Available via the intranet homepage PRACTICAL DEMONSTRATION Safe storage of records Clear documentation Accurate records Assessing pain Incident reporting Up to date charts Lock trolleys Who is who in the trust Confidentiality Keep all informed
How to prepare for a CQC visit Consider the following questions: • Is my mandatory (MAST) training up to date? • Do I keep the information available to patients up to date? • Do I document verbal discussions about care, treatment and support on the patient’s file? • Do I link new patient records with any previous records that exist for that patient? • Do I ensure that all patient records are up to date, accurate, and kept confidential? • Are records stored and transferred securely according to our policy? • Have I completed Record Keeping training? • Do I know where to access all mandatory policies relating to quality, safety and clinical governance?
Quality Inspections: Identified Risks • Nursing documentation to be addressed – Risk assessments incomplete or not reviewed, accuracy and completeness of observations, individualised patient care plan • DNAR notices are not always completed • MUST assessments not always completed on all patients • Escalation as a result of an EWS score are not always well documented • Completion of fluid balance charts and weight charts.
Are we caring? CQC Key Lines of Enquiry • ALL STAFF • What does this mean in your daily practice? • The CQC Inspector can and will approach any staff member including doctors, nurses, managers, hotel services, allied health professionals, administrative staff • If approached or observed by a CQC Inspector would you be able to answer these questions? • Be prepared! What does this mean in your daily practice?
What does this mean in your daily practice? POLICIES AND PROCEDURES • Equality and diversity • Interpreting Service • Complaints • Communicating effectively with patients • End of life care and DNAR • Patient Information • Friends and Family Test • DNAR properly documented and communicated Available via the intranet homepage PRACTICAL DEMONSTRATION Privacy & dignity Tone of voice Attitudes & behaviour Listen to patients Noise at night Support at mealtimes Learning disability/ vulnerable patients Dementia patients End of life care and DNAR Access to Interpreters Intentional rounding
What can you do prior to inspection Consider the following questions: • Do I give relevant information leaflets/contact details to patients? • Do I involve patients in their care plans by explaining their treatment, options and care? • Do I help patients to understand what is going to happen to them and why • Do I give patients information about the risks and benefits of alternative treatments? • Do I effectively communicate with a patient’s relatives to ensure they are involved in the decision-making about the patients care? • Do I document in the patient’s record when they have discussed their treatment options or when they have given them information? • Do patients sign their care plan/assessment to confirm that they have been involved and understand their treatment? • Am I up to date with my Equality and Diversity training? • Does the care environment make patients/families feel safe, comfortable and private? • Do I ensure multi-disciplinary team handovers include all parties to ensure consistence of care – including relatives? • Do I always pull curtains properly around the bed? • Do I always introduce myself ? • Do I always check what patients liked to be called?
Quality Inspections: Identified Risks • On some wards the nursing staff need to be more sympathetic when responding to patients concerns • On some wards patients felt that they had not been involved in their care plans.
Are they responsive? CQC Key Lines of Enquiry • ALL STAFF • What does this mean in your daily practice? • The CQC Inspector can and will approach any staff member including doctors, nurses, managers, hotel services, allied health professionals, administrative staff • If approached or observed by a CQC Inspector would you be able to answer these questions? • Be prepared!
What does this mean in your daily practice? POLICIES AND PROCEDURES • Adverse incidents • Nutrition and hydration • Intentional rounding • Productive ward Available via the intranet homepage PRACTICAL APPLICATION Call bells answered in a timely way Discharge planning Clinical leadership Team working Decision on mental capacity Handing over vital information from shift to shift Staff safety forums Quality rounds Ward information Don’t take your troubles home - resolve concerns and issues proactively
What can you do prior to inspection Consider the following questions: • Do I take account of patients’ needs and wishes so that they are ready to leave hospital at the right time? • Do I provide patients and their families with the sufficient information to leave hospital with? • Do I ensure nutritional and hydration needs are met (red trays, red beakers and water jugs with red lids)? • Do I ensure multi-disciplinary team handovers include all parties to ensure consistence of care – including relatives? • Do I take account of patients needs at each stage of their treatment? • Do I ensure the patient has made adequate arrangements for leaving hospital? • Do I encourage patients to complete patient survey's or signpost to make complaints? • Do I ensure the welfare needs of patients extends beyond the hospital back in to the community?
What does this mean in your daily practice? POLICIES AND PROCEDURES • Supporting Staff • Temporary Staff Available via the intranet homepage PRACTICAL APPLICATION Who is your matron? Who is your head of Nursing/DDNG Tidy ward What are patients saying Assistance at mealtimes White boards above bed
What can you do prior to inspection Consider the following questions: • Have I had an appraisal? • Am I up to date with my MAST training? • How do I keep my knowledge and skills up to date? • Do I know what the trust values are? • What areas of my work am I proud of? • What worries me? How am I addressing my concerns?
Quality Inspections: Identified Risks • Not all staff have had Individual performance reviews
CONCLUSION • We must meet the essential standards, for the sake of our patients • We got much of it right in August • We need to get it right, everywhere, for all of our patients – consistency • This is our responsibility to our patients • This presentation and further resources are available via the intranet homepage