Download
1 / 23
260 likes | 809 Views
Anorectal physiological assessment. Perineal trauma study day 13 th November 2007 Mrs. Kirsty Cattle MRCS Research Registrar. Faecal incontinence. Causes of incontinence Stool factors Stool delivery Rectum – storage organ Anal sphincters Anatomical Innervation Miscellaneous.

E N D
Anorectal physiological assessment Perineal trauma study day 13th November 2007 Mrs. Kirsty Cattle MRCS Research Registrar
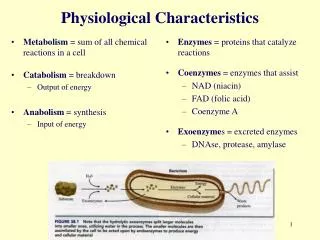
Faecal incontinence • Causes of incontinence • Stool factors • Stool delivery • Rectum – storage organ • Anal sphincters • Anatomical • Innervation • Miscellaneous
Anorectal physiology • Manometry • Including anorectal inhibitory reflex • Rectal sensation • PNTML • Pudendal nerve terminal motor latency • Endoanal ultrasound
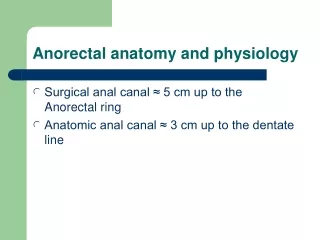
Resting pressure • Reflects internal anal sphincter function • Normal: > 45 cm H2O, usually ~ 70 cm H2O • Difference between maximum resting anal pressure and rectal pressure
Pressure (cm H2O) Maximum resting pressure Distance from anal verge (cm)
Squeeze pressure • Reflects external anal sphincter function • Normal in women: ~ 70 cm H2O • The “best squeeze” is documented as the maximum squeeze pressure, i.e. the biggest increase generated from resting anal pressure
Pressure (cm H2O) Maximum squeeze pressure Distance from anal verge (cm)
Anorectal inhibitory reflex • Reflex relaxation of the internal anal sphincter when the distal rectum is distended
Inflation of balloon in rectum with 20-30 ml air Rectal balloon deflated Pressure (cm H2O) Time
Rectal sensation • Normal values: • First sensation 40 – 50 ml • Call to stool 80 – 100 ml • Urgency 120 – 150 ml
Pudendal nerve studies • Measurement of conduction speed in terminal pudendal nerve • Transrectal technique: Stimulate nerve near ischial spines, measure time taken to produce twitch of external anal sphincter • Normal range < 2.2 ms • Statistically different between incontinent patients and controls, but may be normal in incontinent patients
http://med.stanford.edu/interactiveimages/anatomyweb/media/PL/M/0006/035.gif
http://www.alpinebiomed.com/modules/cms/UserFiles/Image/accessories/StMarks9013L4401.jpg
Ultrasound • 10 MHz rotating probe • Clear visualisation of sphincters • Delineation of simple fistulae
http://radiology.rsnajnls.org/cgi/content/figsonly/224/2/417
http://radiology.rsnajnls.org/cgi/content/figsonly/224/2/417
Other assessments • Barium enema/Colonoscopy • Defaecating proctogram
Summary • Anorectal physiology studies provide us with: • Function and anatomy of sphincters • Assessment of sensation • Estimation of pudendal nerve function • Use: • Treatment options, including planning of surgery
Thank you • Any questions?