Download
1 / 10
150 likes | 557 Views
Muscle Disease. Neurology Rotation Lecture Series Last Updated by Lindsay Pagano Summer 2013. Case Presentation. A 5 year old male is brought to your office because his mother noted that he has difficulty with activities that other children in his Kindergarten class can do well.

E N D
Muscle Disease Neurology Rotation Lecture Series Last Updated by Lindsay Pagano Summer 2013
Case Presentation A 5 year old male is brought to your office because his mother noted that he has difficulty with activities that other children in his Kindergarten class can do well. • Sat up at 10 months, began to walk at 18 months • Now cannot stand or hop on one foot • Runs awkwardly, fatigues easily, difficulty walking up stairs • Behind in learning the alphabet, colors and numbers • Term SVD, no complications • No FHx of neurologic disease • PE: normal except for • Musculoskeletal: • Mild lordosis • Bilateral heel cord tightness • Mildly enlarged calves • Neuro: • Mild diffuse hypotonia • Trouble lifting neck from table; BLE > BUE weakness • DTRs 1+ diffusely Differential? Diagnosis?
Duchenne Muscular Dystrophy • X-linked recessive, 1:3300 males • Xp21, dystrophin gene mutation (2/3 familial, 1/3 new mutations) • Typically presents at 5 years old • difficulty running • abnormal gait (waddling) • historic motor delay • PE • Musculoskeletal • lumbar lordosis • calf pseudohypertrophy (muscle fibers replaced with fat and connective tissue • Neurologic • Neck flexor weakness • Symmetric and proximal UE and LE weakness, LE > UE • Diffuse hypotonia, DTRs 1+ diffusely
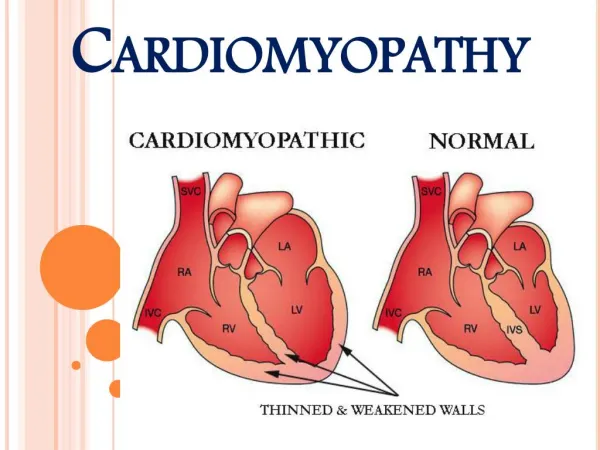
DMD, continued • Other system involvement • Dystrophin is found in skeletal muscle, smooth muscle, cardiac muscle and brain • May have cognitive impairment • All develop cardiomyopathy • May develop intestinal pseudo-obstruction • Gower Sign • Diagnosis • CK elevated (10x upper limit normal) • Muscle biopsy (absent dystrophin) • Genetic/DNA testing • +/- EMG/NCV • Prognosis • Supportive care • +/- steroids • Wheelchair bound by 13 years old • Death in 20s from respiratory or cardiac failure
Becker Muscular Dystrophy • Same pathogenesis as DMD • Except for inframe mutations for BMD, out of frame for DMD • Slower course • Present between 5-15 years old • Wheelchair bound after 16 years old • Live through their 30s-40s • Less severe course, less likely to have • Cognitive impairment • Cardiac disease • Contractures • Scoliosis • GI issues • CK elevated (5x upper limit of normal) • Muscle biopsy with decreased dystrophin
Congenital Muscular Dystrophy • AR, heterogeneous group of disorders, classic or syndromic • Presents at birth or in infancy • Presents with • Weakness • Poor feeding • Respiratory difficulties • Neuro exam • Hypotonia • Diffuse weakness • Other findings • Arthrogryposis • +/- CNS involvement • +/- cardiac involvement • Diagnosis • CK elevated • Muscle biopsy consistent with myopathy or dystrophic process
Congenital Myotonic Dystrophy • > 1000 CTG repeats in the DMPK gene, 19q13.3 (anticipation), AD • Mom is typically the affected parent (check her grip!) • Poor fetal movement, polyhydramnios • Feeding and respiratory difficulties, cognitive impairment, developmental delay • Neuro PE: • Facial diplegia • Hypotonia • Decreased DTRs • Other PE: • Joint deformities, from clubfoot to arthrogryposis • No clinical or EMG myotonia until 2 years of age • Genetic testing
SMA See the hypotonia lecture!
PREP question A 6 year old girl presents to the emergency department with a facial rash, fatigue and muscle pain. She has been previously healthy. On PE, you note an erythematous rash over her cheeks and eyelids, and papules over her knuckles. Her muscles are tender to palpation. With encouragement, her grip strength is normal, but her strength seems diminished on shoulder abduction. She has difficulty standing from a seated position. Of the following, the MOST likely cause for this child’s symptoms is: • Dermatomyositis • Duchenne muscular dystrophy • Polymyositis • Systemic lupus erythematosus • Viral myositis
A. dermatomyositis Dermatomyositis • Inflammatory myopathy • Initial symptoms is typically rash, but weakness may also present/go unnoticed initially (symmetric and proximal) • Skin: periorbitalviolaceous erythema (heliotrope rash), Gottron papules over DIPs, violaceous discoloration over extensor surfaces of knee and elbows • Evaluate for cardiac involvement • Labs: CK (may be normal initially), ESR (may be normal initially), ANA with speckled pattern, lymphopenia • Imaging: fat-suppression MRImuscle • Tx: immunosuppression • Regarding the other choices: B. Duchennes: Xlinked, no rash C. polymyositis: no derm findings D. SLE: does not have this kind of rash E. viral myositis: does not have this kind of rash